
![]()
May–Thurner syndrome
May–Thurner syndrome (MTS), also known as iliac vein compression syndrome or Cockett syndrome, is a vascular condition resulting from chronic compression of the left common iliac vein (LCIV) by the overlying right common iliac artery (RCIA) against the fifth lumbar vertebra.
This mechanical compression predisposes the vessel to endothelial injury, venous spur formation, and ultimately iliofemoral deep vein thrombosis (DVT). Though often asymptomatic, MTS is a significant cause of unilateral left leg swelling and DVT, particularly in young women.
Anatomical variants are relatively common, with cadaveric and radiological studies showing LCIV compression in up to 22–32% of individuals. However, symptomatic MTS accounts for only 2–5% of all lower extremity DVTs. Clinical presentation ranges from chronic venous insufficiency to sudden-onset phlegmasia cerulea dolens.
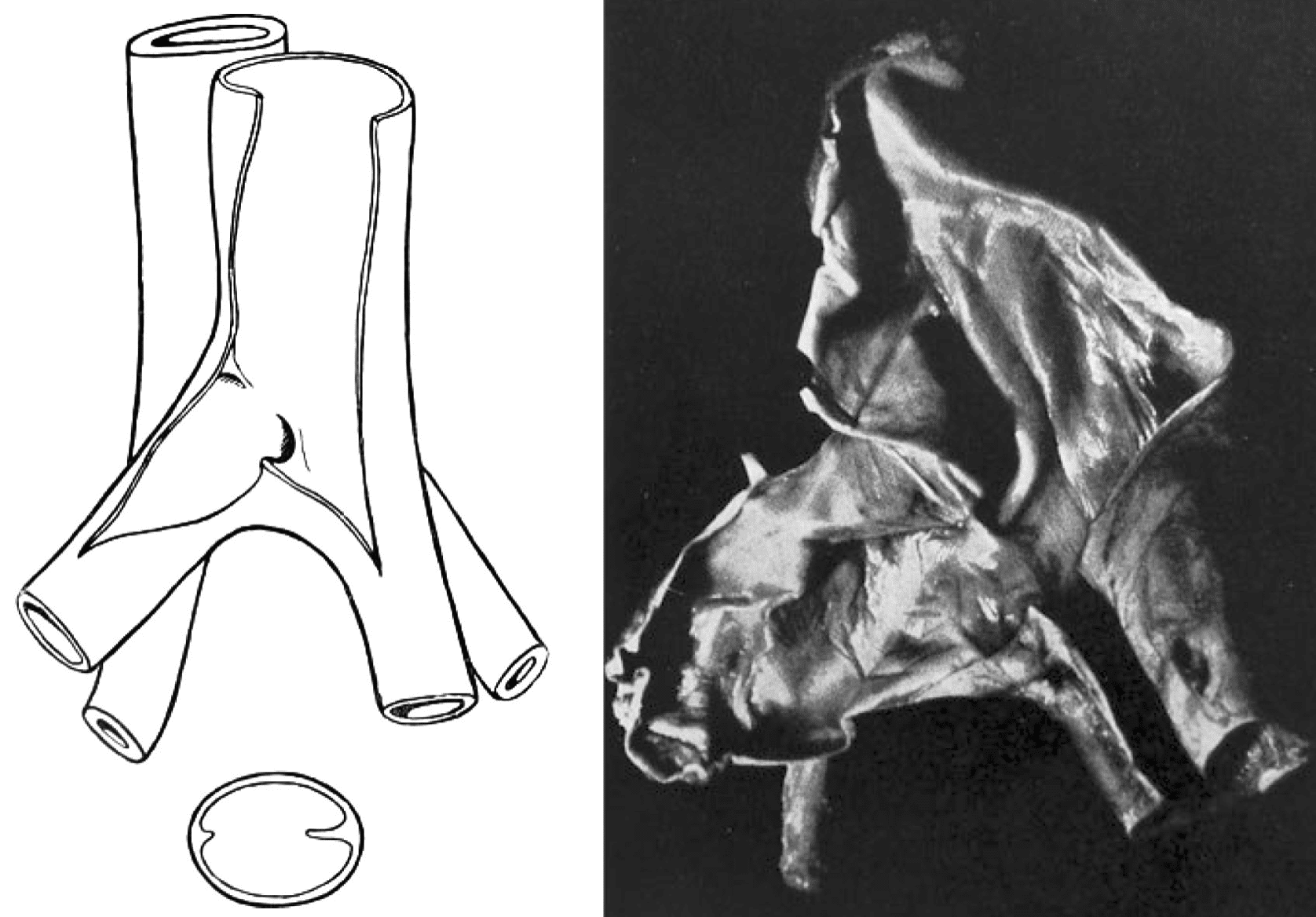
The eponym originates from Robert May (1912-1984) and Josef Thurner (b. 1927) who first published their detailed anatomical and histological findings in 1956/1957, identifying intraluminal “spurs” in 22% of 430 cadavers. Though Virchow had earlier observed the predilection for left-sided DVT in 1851, May and Thurner provided the anatomical rationale and linked it directly to the formation of venous thrombi.
MTS remains clinically relevant in emergency, vascular, and interventional radiology settings, and it features prominently in venous thromboembolism (VTE) workups, especially in idiopathic or recurrent DVT.
History of May–Thurner syndrome
1851 – Rudolf Virchow (1821–1902) identifies a left-sided predominance in iliofemoral DVT during autopsy studies. Postulates a mechanical flow obstruction by crossing arteries.
1908 – James Playfair McMurrich (1859–1939) reports congenital adhesions in the LCIV, associating them with femoral and iliac vein thrombosis.
1943 – Ehrich and Krumbhaar describe obstructive abnormalities in 23.8% of LCIVs during autopsy, supporting the idea of acquired pathologies.
1953–1956 – Robert May and Josef Thurner conduct extensive autopsy work at the University of Innsbruck. Their preliminary reports identify venous narrowing due to arterial compression.
1957 – May and Thurner publish “The cause of the predominantly sinistral occurrence of thrombosis of the pelvic veins” in Angiology. In 430 cadaver dissections, they report characteristic “spurs” in 22%, histologically composed of fibrous tissue due to repetitive arterial pulsations. Term “May–Thurner syndrome” later adopted.
1965 – Frank Bernard Cockett and M. Lea Thomas clinically correlate left-sided iliofemoral DVT with LCIV compression in surgical patients, calling it “iliac compression syndrome”.
2000s–present – Increased awareness through MRV/CT angiography and intravascular ultrasound. MTS incorporated into broader classification systems (eg. S-V-P CEAP) and increasingly treated with endovascular stenting.
Key Contributors
- Rudolf Virchow (1821–1902) – Early observer of left-sided DVT predominance.
- James P. McMurrich (1859–1939) – First documented congenital LCIV adhesions in 1908.
- Frank Bernard Cockett (1916-2014) – British surgeon who described the syndrome clinically and proposed surgical management.
- Robert May (1950s) – Austrian vascular pathologist; co-authored foundational autopsy studies on venous spurs.
- Josef Thurner (1950s) – Collaborator with May; provided histologic detail and classification of spurs.
Alternative names
- Cockett syndrome
- iliac vein compression syndrome
References
Historical references
- McMurrich JP. The occurrence of congenital adhesions in the common iliac veins and their relations to thrombosis of the femoral and iliac veins. The American Journal of the Medical Sciences, 1908, 135:342.
- May R, Thurner J. Ein Gefässporn in der Vena iliaca communis sinistra als Ursache der überwiegend linksseitigen Beckenvenenthrombosen [A vascular spur in the vena iliaca communis sinistra as a cause of predominantly left-sided thrombosis of the pelvic veins]. Z Kreislaufforsch. 1956 Dec;45(23-24):912-22.
- May R, Thurner J. The cause of the predominantly sinistral occurrence of thrombosis of the pelvic veins. Angiology. 1957 Oct;8(5):419-27.
- May R. The cause of predominantly sinistral occurrence of thrombosis of the pelvic veins. Minerva Cardioangiol Eur. 1957 Oct-Dec;3(4):346-9.
- Cockett FB, Thomas ML. The iliac compression syndrome. Br J Surg. 1965 Oct;52(10):816-21.
- Cockett FB, Thomas ML, Negus D. Iliac vein compression.–Its relation to iliofemoral thrombosis and the post-thrombotic syndrome. Br Med J. 1967 Apr 1;2(5543):14-9.
- Cockett FB. Venous causes of swollen leg. Br J Surg. 1967 Oct;54(10):891-4.
Eponymous term review
- Cunningham K. Abdominal Imaging Cases 012. LITFL
- Ho AMH, Chung AD, Mizubuti GB. A hairdresser’s painful swollen left leg: artery compresses vein in May-Thurner syndrome. Lancet. 2019 Oct 26;394(10208):e33
- Harbin MM, Lutsey PL. May-Thurner syndrome: History of understanding and need for defining population prevalence. J Thromb Haemost. 2020 Mar;18(3):534-542.
- Junianto I, Zuhri E, Andriantoro H, Indriani S, Siddiq T, Adiarto S. May-Thurner Syndrome: A Forgotten Cause of Deep Vein Thrombosis. Int J Angiol. 2022 Nov 2;34(2):122-125.
- Armenta-Flores R. May-Thurner diagnosis and management. Phlebolymphology. 2022;29(3):5–13.
- Mangla A, Hamad H. May-Thurner Syndrome. 2024 Mar 11. In: StatPearls
- Silverstone L. May-Thurner syndrome. Radiopaedia
eponymictionary
the names behind the name