
![]()
Acid and Alkali Burns to the Eye
Chemical injuries to the eye are true ocular emergencies requiring immediate saline irrigation, category 2 triage, and urgent ophthalmology consultation.
Introduction
- Ophthalmology consultation is mandatory for all cases.
- Chemical eye injuries are true ocular emergencies.
- Assign Category 2 triage status.
- Immediate saline irrigation is essential.
Pathophysiology
Alkali Burns
- Cause liquefactive necrosis.
- Tissue destruction continues until the agent is completely removed.
- Alkalis (and hydrofluoric acid) are more damaging than acids.
Acid Burns
- Typically cause coagulative necrosis, which limits tissue penetration (except for HFl).
Prognosis Factors
Recovery depends on:
| Factor | Description |
|---|---|
| Causative agent | Type and strength of the chemical |
| Limbal involvement | Assessed in “clock hours” |
| Conjunctival damage | Measured by % of surface area affected |
| Corneal damage | Degree of opacity and clarity |
Clinical Assessment
General Notes
- Immediate treatment before full examination is vital.
- Injury severity increases with duration of exposure.
History
- Time and mechanism of injury
- Type and concentration of chemical
- First aid measures and timing
Examination
- Blepharospasm indicates more severe injury.
- Corneal clarity suggests lesser damage.
- Assess vascular blanching, especially at the limbus.
- Record visual acuity in both eyes (if possible).
Classification of Severity
- The modified Roper-Hall classification (Dua et al.) grades injuries from 1 to 6.
- Based on Limbal involvement (clock hours) and Conjunctival involvement (% of surface)
| Grade | Prognosis | Clinical Findings | Conjunctival Involvement | Analogue Scale* |
|---|---|---|---|---|
| I | Very good | 0 clock hours of limbal involvement | 0% | 0 / 0% |
| II | Good | ≤3 clock hours of limbal involvement | ≤30% | 0.1–3 / 1–29.9% |
| III | Good | >3–6 clock hours of limbal involvement | >30–50% | 3.1–6 / 31–50% |
| IV | Good to guarded | >6–9 clock hours of limbal involvement | >50–75% | 6.1–9 / 51–75% |
| V | Guarded to poor | >9–<12 clock hours of limbal involvement | >75–<100% | 9.1–11.9 / 75.1–99.9% |
| VI | Very poor | Total limbus (12 clock hours) involved | Total conjunctiva (100%) involved | 12 / 100% |
*Analogue scale records the limbal involvement in clock hours of affected limbus/percentage of conjunctival involvement. While calculating percentage of conjunctival involvement, only involvement of bulbar conjunctiva, up to and including the conjunctival fornices is considered.
Management
1. Analgesia
- Immediate use of local anaesthetic drops
- Repeat as necessary
- IV opioids and antiemetics if severely distressed
2. Irrigation
- Use isotonic saline immediately
- Minimum 30–40 minutes for severe injuries
- Start with at least 1 litre, even if prior irrigation attempted
- Morgan lens may assist
- Evert eyelids to irrigate inner surfaces
3. pH Monitoring
| Tool | Notes |
|---|---|
| Universal Indicator Paper | Test forniceal space (not just saline) |
| Acceptable pH | 6.5–8.5 (normal is ~8) |
| Ensure dryness | Dry eye before pH test to avoid saline contamination |
4. Removal of Residual Particles
- Use cotton bud to remove visible debris
5. Topical Antibiotics
- Start empiric topical antibiotics
6. Mydriatics
Used for pain relief and to prevent posterior synechiae (refer to Therapeutic Guidelines for prescribing details.)
| Drug | Duration |
|---|---|
| Tropicamide 0.5% | ~6 hours |
| Cyclopentolate 0.5% | ~24 hours |
| Homatropine 2% | Up to 5 days |
7. Topical Steroids
- Only on advice of ophthalmologist
8. Surgical Management
- Severe cases may require corneal grafting
- Prognosis depends on initial severity
Additional Measures (Ophthalmology-directed)
- Topical Vitamin C
- Topical Citrate
Disposition
- All patients require urgent ophthalmology consultation
- Severe burns → likely admission and urgent review
Appendix 1
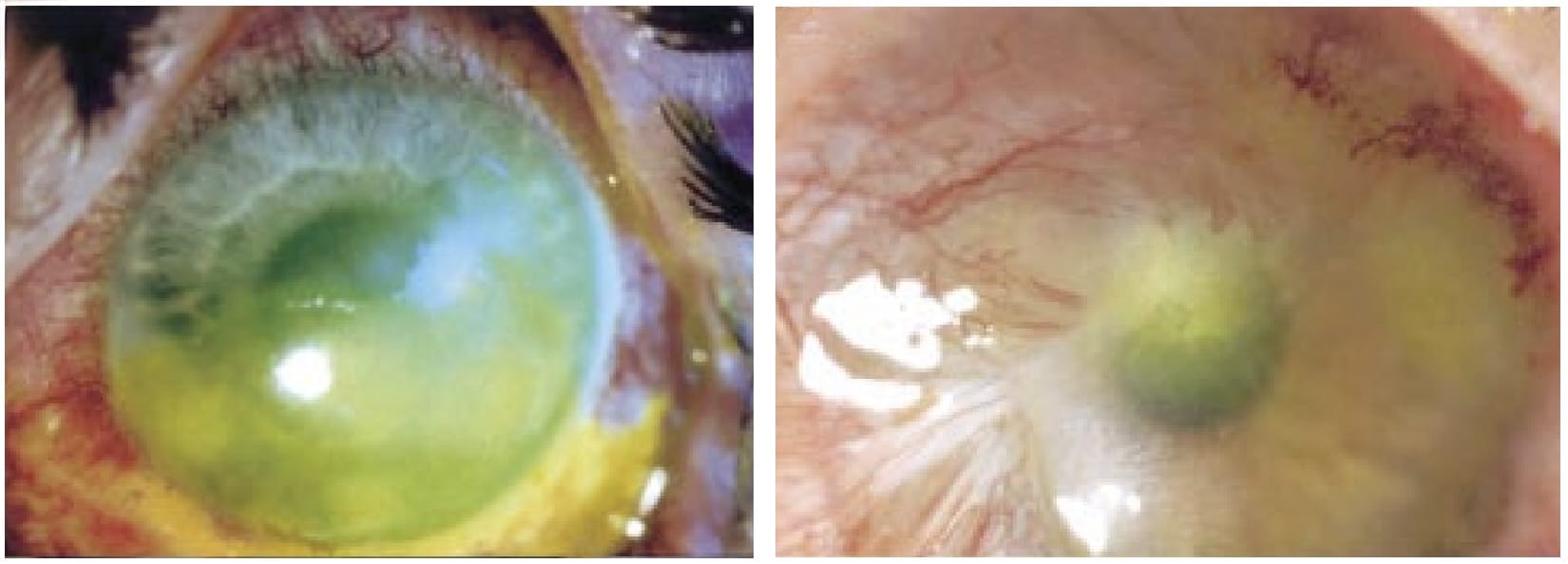
Left: Grade 3 (5/35%) ocular surface burn with industrial alkali. Five clock hours of the limbus and 35% of the conjunctiva were involved.
Right: Grade 5 (9.5/60%) ocular surface burn following alkali injury. Nine and a half clock hours of the limbus and 60% of the conjunctiva were involved. Dua 2001
Appendix 2
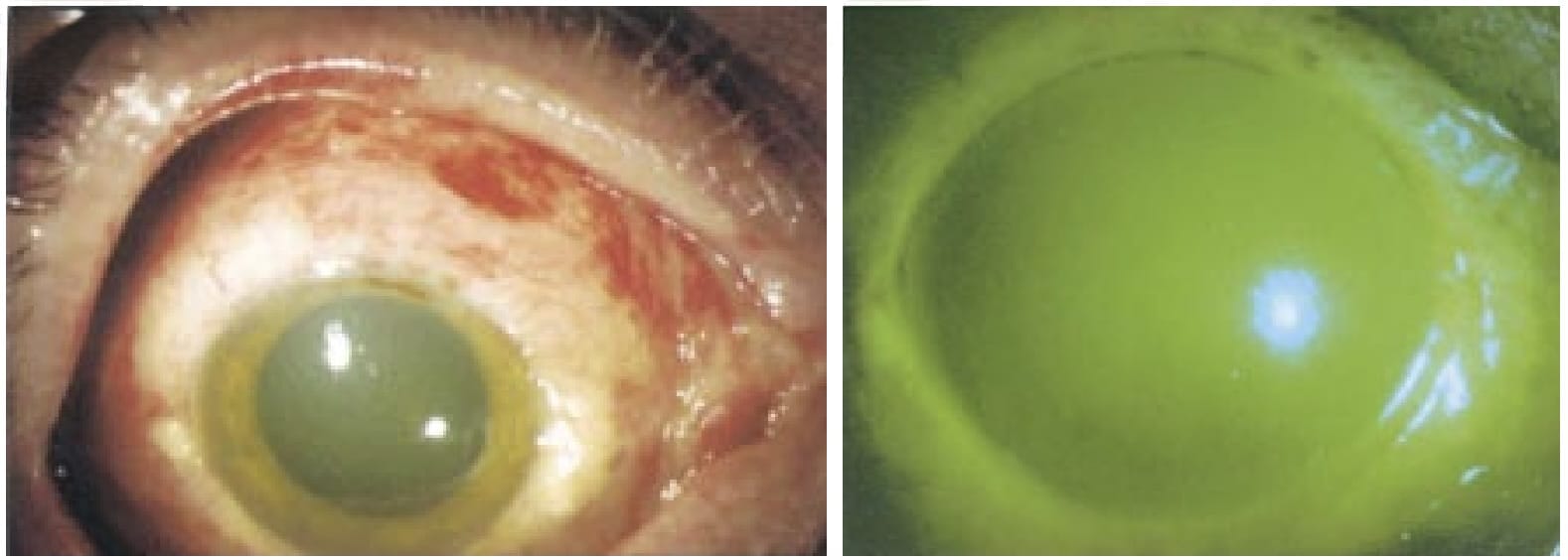
Grade 6 (12/100%) ocular surface burn. The entire limbus and the entire conjunctiva were involved. Left: Diffuse view showing involvement of the entire upper and lower bulbar conjunctiva. Right: The entire corneal surface and 12 clock hours of the limbus are involved. Very poor prognosis. Dua 2001
References
FOAMed
- Nickson C. Ophthalmology Befuddler. Clinical Cases. LITFL
- Nickson C. The Eye In Chemical. LITFL
Publications
- Roper-Hall MJ. Thermal and chemical burns. Trans Ophthalmol Soc U K (1962). 1965;85:631-53.
- Dua HS, King AJ, Joseph A. A new classification of ocular surface burns. Br J Ophthalmol. 2001 Nov;85(11):1379-83.
- The Eye Emergency Manual, NSW Department of Health, 3rd ed. 2023
Fellowship Notes

Ba(Hons) Sheffield University, MBBS Newcastle University, MRCEM. UK Emergency Medicine doctor working in Australia |Stronger Medicine|

Educator, magister, munus exemplar, dicata in agro subitis medicina et discrimine cura | FFS |