
![]()
Epley manoeuvre
Description
A particle repositioning manoeuvre for the treatment of BPPV – with the aim of moving the canaliths out of the posterior semicircular, back into the utricle. It have been shown to be safe and can be effective at resolving BPPV in 50-85% of cases (2014, 2013).
The original manoeuvre was first described by John Epley in 1980 also involved vibrations over the mastoid during the manoeuvre. Today the Modified Epley is performed without the vibrations.
How to perform the Modified Epley Manoeuvre
They Epley maneuver for right sided BPPV:
- The patient sits upright and turns head 45° towards the right (affected ear)
- Keeping their head turned the patient lies back and hangs their head off the end of bed to extend the neck to around 20degrees beyond horizontal, supported by the examiner
- Hold this position for 30sec, until the nystagmus and vertigo has resolved
- Keeping the head extended rotate the head to 45° to the left
- Hold this position for 30sec, until the nystagmus and vertigo has resolved
- Keeping the head turned at 45°, roll the whole body onto the left side so that the patient is now looking down at the floor
- Hold this position for 30sec, until the nystagmus and vertigo has resolved
- Keeping the head turned to 45° left, sit the patient up
- Return the head to the midline and tilt it forwards to around 30° so the patient is looking slightly down
The maneuver can be repeated until symptom resolution. It should be performed in the opposite direction for left sided BPPV with the head turning to the left side in the initial step.
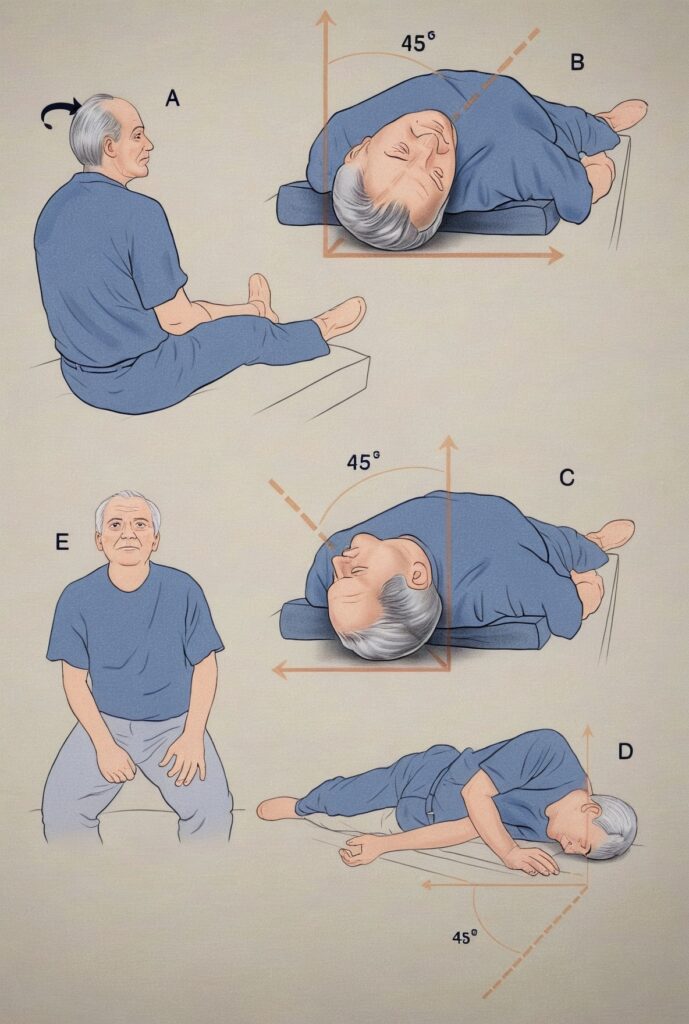
- A. Position the patient on bed with head slightly extended and turned 45 degrees to the right.
- B. Position the patients with head over a pillow placed at shoulder level (as for a normal Dix-Hallpike manoeuvre) and wait one minute.
- C. Turn the head through 90 degrees and wait another minute.
- D. Turn head through a further 90 degrees, while the patient rolls on to the left side and wait another minute.
- E. Sit patient up slowly.
See clinical case for an animation of the manoeuvre, or see below for a longer video on BPPV and the Epley manoeuvre directed and featuring John Epley himself (see 39m15s for animation of the manoeuvre).
Canalithiasis Theory
Epley proposed the canalithiasis theory in 1980 in his paper New dimensions of benign paroxysmal positional vertigo, contrasting with Cupulolithiasis (Schuknecht, 1962). Cupulolithiasis and canalithiasis are two distinct theories that explain the mechanisms behind Benign Paroxysmal Positional Vertigo (BPPV).
Cupulolithiasis refers to otoconia (calcium carbonate crystals normally found in the utricle of the inner ear) adhering to the cupula, a gel-like structure within the semicircular canals. This adhesion causes the cupula to become heavier and more sensitive to gravity, leading to abnormal deflection during head movements. As a result, the affected individual experiences vertigo and nystagmus (involuntary eye movement) because the brain receives incorrect signals about the head’s position in space
Canalithiasis describes the scenario where otoconia are free-floating within the semicircular canals. When the head moves, these particles move through the canal, displacing the endolymph and causing the cupula to deflect. This deflection leads to an inappropriate excitation or inhibition of the vestibular nerve, which is responsible for transmitting balance information to the brain. The movement of the otoconia through the canal results in a transient and intense episode of vertigo, typically lasting less than a minute.
The distinction between these two conditions is crucial for determining the appropriate treatment. For example, the Epley manoeuvre is commonly used to treat canalithiasis by guiding the free-floating otoconia back to the utricle, where they can be reabsorbed.
Associated Persons
- John McNaughton Epley (1930-2019)
Alternative names
- Epley manoeuvre
- Modified Epley
- Canalith repositioning manuever
Controversies
Epley faced over a decade of scepticism and ridicule from peers in his field who did not believe in his repositioning manoeuvre, before it was widely accepted.
References
Original articles
- Epley JM. New dimensions of benign paroxysmal positional vertigo. Otolaryngol Head Neck Surg. 1980; 88(5): 599-605.
Epony review
- Parnes LS, Agrawal SK, Atlas J. Diagnosis and management of benign paroxysmal positional vertigo (BPPV). CMAJ. 2003;169(7):681-693.
- Prokopakis E, Vlastos IM, Tsagournisakis M, Christodoulou P, Kawauchi H, Velegrakis G. Canalith repositioning procedures among 965 patients with benign paroxysmal positional vertigo. Audiol Neurootol. 2013;18(2): 83-88
- Hilton MP, Pinder DK. The Epley (canalith repositioning) manoeuvre for benign paroxysmal positional vertigo. Cochrane Database of Systematic Reviews 2014; 12: CD003162
eponymictionary
the names behind the name

Studied at Univerisity of Cambridge - BA MB BChir. British doctor working in emergency medicine in Perth, Australia. Special interests include primary care and emergency medicine.
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |