
![]()
Superficial venous thrombosis
Superficial venous thrombosis is rarely life-threatening. It carries a low risk of pulmonary embolism (~<1% in untreated patients), but the concurrent incidence of underlying DVT is notable (~25%).
The term phlebitis refers to the presence of inflammation within a vein, whereas thrombosis indicates the presence of clot.
The term thrombophlebitis is used broadly in the literature and often refers to venous inflammation even when it is unclear whether thrombosis of the vein has occurred. In the lower extremity, superficial phlebitis is commonly associated with venous thrombosis.
Here we review primarily superficial venous thrombosis.
Superficial venous thrombosis is rarely life-threatening. It carries a low risk of pulmonary embolism (~<1% in untreated patients), but the concurrent incidence of underlying DVT is notable (~25%).
A thorough diagnostic evaluation is essential because:
- Superficial thrombosis may extend to become deep (increasing PE risk).
- There may be significant underlying pathology (risk factors similar to DVT).
Efforts should be made to prevent progression to the deep veins, as this can cause chronic deep venous insufficiency and PE.
The greatest risk of extension occurs in cases involving the great saphenous vein above the knee, especially near the saphenous-femoral junction.
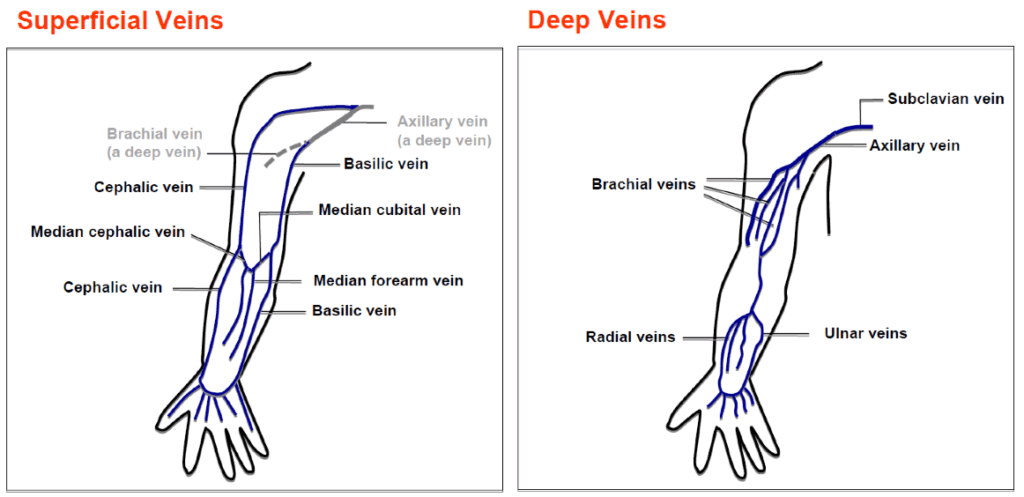
Anatomy
The venous drainage system of the upper limb is divided into:
- Superficial system (runs with lymphatics)
- Deep system (runs with deep arteries)
Pathophysiology
Superficial thrombophlebitis results from inflammation and/or thrombosis, and less commonly infection of the vein.
It should be assumed to involve deep veins until proven otherwise.
Risk factors (in addition to DVT risk factors):
- Local trauma (e.g. cannulations)
- Varicosed veins
- Stasis
- IV drug use
- IV therapeutic drugs
Complications
- Extension into deep venous system
- Low risk in upper limbs
- Higher risk in great saphenous vein above the knee
- Associated DVT (~25%)
- May be simultaneous and in different limbs
- Secondary infection (septic thrombophlebitis)
Clinical Features
Normal veins may be visible at the foot/ankle but not typically elsewhere. Dilated superficial leg veins above the ankle suggest pathology.
Signs of thrombosed superficial veins:
- Tenderness
- Swelling
- Induration
- Erythema/fever (if infected)
Progression: develops over hours to days and resolves over days to weeks. An indurated cord may persist for months.
Thorough assessment should include evaluation for underlying malignancy.
Differential Diagnoses
- Cellulitis
- Lymphangitis
- DVT
- Suppurative thrombophlebitis
- High fever, fluctuance, purulent drainage
- Consider if erythema extends beyond the vein
- Often iatrogenic (e.g. cannulation)
Investigations
Blood Tests
Directed by clinical suspicion:
- FBE
- CRP
- U&Es / Glucose
- Coagulation profile
- Biopsy (select cases e.g. vasculitis)
Ultrasound
Used to:
- Confirm diagnosis
- Rule out DVT (including contralateral limb)
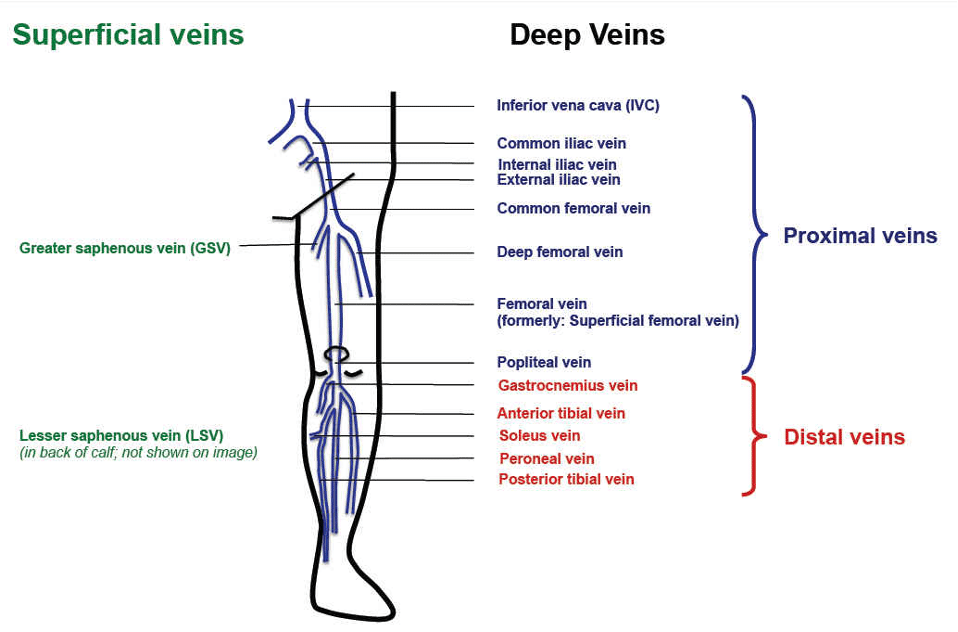
Note: The term “superficial femoral vein” is misleading. It is a deep vein. Misinterpretation can lead to fatal errors.
MRI
Magnetic Resonance Venography (MRV) is more sensitive than ultrasound and detects alternate pathologies.
Management
Initial ED priorities:
- Rule out associated DVT
- Rule out PE
- Rule out septic thrombophlebitis
Anticoagulation vs Antiplatelet Therapy
Cases requiring anticoagulation:
- Thrombosis within 1 cm of deep venous system:
- Sapheno-popliteal junction
- Sapheno-femoral junction
- Cephalic vein extending into axillary vein
- Significant thrombosis risk factors:
- Active malignancy
- Prior thrombosis
- Procoagulant disorders
- Recurrent episodes
For extensive thrombosis (>5 cm) or significant symptoms, consider prophylactic anticoagulation for 2–6 weeks (liaise with Haematology).
Note: NOACs are not indicated for superficial thrombosis.
Indefinite anticoagulation is generally not recommended.
Cases not requiring full anticoagulation:
- Treat with NSAIDs or antiplatelet agents
- Monitor for extension
- Repeat ultrasound in 7–10 days
Antibiotics
Indicated if suppurative thrombophlebitis is suspected. Consider:
- Antibiotics
- Surgical drainage
- Vein excision
Surgery
Surgical interruption of the saphenofemoral junction is rarely done today. May be considered in:
- Absolute contraindication to anticoagulation
Disposition
- Early Haematology consultation if anticoagulation requirement is unclear
References
Publications
- Balahura AM, Florescu AG, Barboi TM, Weiss E, Miricescu D, Jurcuț C, Jinga M, Stanciu S. Current Diagnostic and Therapeutic Challenges in Superficial Venous Thrombosis. Medicina (Kaunas). 2024 Sep 6;60(9):1466.
- Scheres LJJ, Lijfering WM, Cannegieter SC. Current and future burden of venous thrombosis: Not simply predictable. Res Pract Thromb Haemost. 2018 Apr 17;2(2):199-208.
FOAMed
Fellowship Notes
Physician in training. German translator and lover of medical history.

Educator, magister, munus exemplar, dicata in agro subitis medicina et discrimine cura | FFS |