
![]()
Achille Mario Dogliotti
Achille Mario Dogliotti (1897-1966) was an Italian surgeon
Dogliotti was a versatile surgeon-scientist whose work spanned anaesthesia, pain therapy, general and cardiac surgery. Trained as a surgeon, he approached anaesthesia and analgesia as integral components of operative care rather than separate disciplines.
Dogliotti made contributions to neuraxial blockade, particularly through his development of segmental epidural (peridural) anaesthesia in the early 1930s. He demonstrated that controlled, regional blockade could be achieved by injecting local anaesthetic into the epidural space at lumbar or thoracic levels, avoiding many of the haemodynamic and meningeal complications of spinal anaesthesia. His description of the loss-of-resistance technique for identifying the epidural space (“Dogliotti’s principle”) transformed epidural anaesthesia into a reproducible and widely adoptable procedure.
Dogliotti was a pioneer of pain therapy, employing chemical neurolysis and alcoholisation of posterior nerve roots and cranial ganglia for refractory neuralgia. From the late 1940s he also emerged as a leader in Italian cardiac surgery, founding a dedicated centre in Turin and, on August 7, 1951, reporting one of the earliest successful human operations using total extracorporeal blood circulation.
Biographical Timeline
- Born September 25, 1897, Turin, Italy. Son of Luigi Dogliotti, physician and mayor of Alba, and Clotilde Ferrara Bardile
- 1914 – Entered the Faculty of Medicine, University of Turin
- 1915–1918 – Volunteered for military service during World War I. Served initially as medical orderly, then medical officer. Awarded two War Crosses for bravery
- 1920 – Graduated in Medicine, University of Turin. Doctoral thesis: Splenectomy in haemolytic jaundice. Appointed intern at the Institute of Surgical Pathology, Turin, under Ottorino Uffreduzzi (1881–1943)
- 1923 – Appointed Assistant in Surgical Pathology, University of Turin
- 1925–1929 – Advanced surgical training abroad. Study visits to France (Lyon, Paris) and the United States (major surgical centres). Early experimental work on shock, blood transfusion, renal vascularisation, and pain
- 1926 – Achieved libera docenza (habilitation) in Surgical Pathology
- 1933 – Described the peridural segmental anaesthesia technique. Formulated Dogliotti’s principle (loss of resistance for epidural space identification)
- 1935 – Appointed Professor of Surgical Pathology, University of Modena. Research in anaesthesia, pain therapy, and neurosurgery
- 1937 – Appointed Professor of Clinical Surgery, University of Catania. Built and directed a major surgical centre
- 1942 – Volunteered for Second World War service. Served as consultant army surgeon on the Eastern Front. Founded and organised a large Italian military hospital at Voroshilovgrad (Luhansk)
- 1943 – Appointed Professor and Director of Clinical Surgery, University of Turin
- 1946 – Visit to the United States and met with Alfred Blalock (1899–1964)
- 1951 – Founded the Blalock Cardiac Surgery Centre, Turin
- August 1951: Performed the first successful human operation using total extracorporeal circulation
- 1952 – Performed mitral commissurotomy and further pioneering cardiac procedures
- 1956 – Led the Italian medical relief mission into Soviet-invaded Hungary
- 1961 – Presided over medical events linked to the Centenary of Italian Unification (Turin)
- 1964 – Awarded Honorary Citizenship of Alba
- 1965 – Underwent neurosurgery in Zurich for a frontal lobe tumour
- Died June 2, 1966 (age 68 years), in Turin, Italy
Key Medical Contributions
Contributions to neuraxial blockade and Dogliotti’s principle
Dogliotti was central to the modernisation and international adoption of epidural anaesthesia, transforming it from a variably effective procedure into a reproducible, anatomically grounded technique. His work in the early 1930s consolidated epidural blockade as a distinct neuraxial modality, capable of producing controlled, segmental anaesthesia without entering the subarachnoid space.
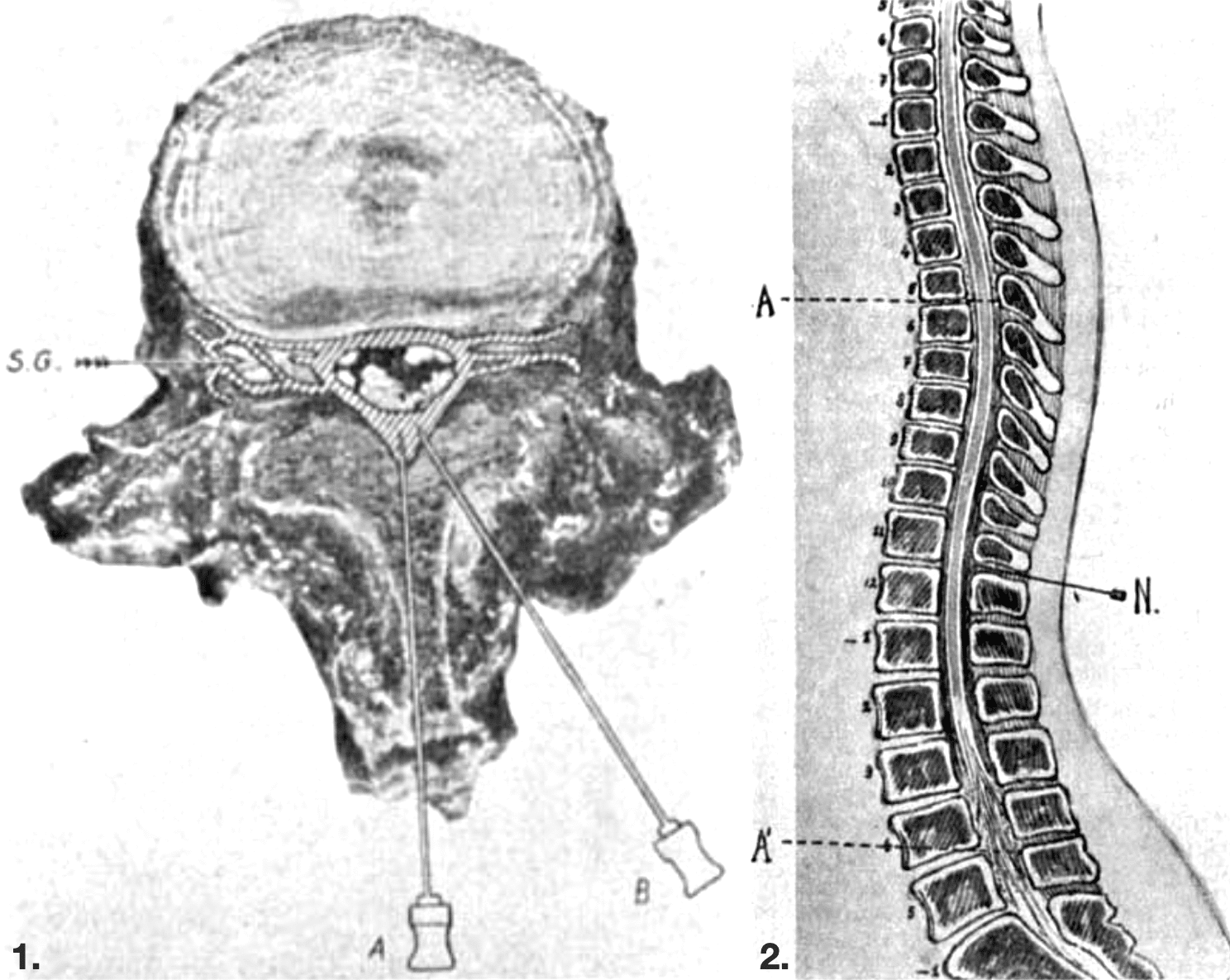
2. Sagittal section of the spinal column showing cranio-caudal diffusion of local anaesthetic within the epidural space, producing controlled segmental blockade without intrathecal injection. [A-A1 = diffusion of anaesthestic; N = needle in epidural space] Dogliotti 1933
Dogliotti described segmental peridural anaesthesia with the injection of local anaesthetic into the epidural space so that it could act on spinal nerves along their course “between the dura mater and the intervertebral canals”. He determined this method would be “an intermediate position between the Corning–Bier method of spinal anesthesia and paravertebral anesthesia”, allowing safe and targeted blockade of selected spinal segments.
With this method one can anesthetize a series of spinal nerves… without danger of diffusion of the anesthetic toward the bulb, of serious fall of blood pressure and without the occurrence of meningeal irritation.
Dogliotti 1933
Dogliotti’s principle
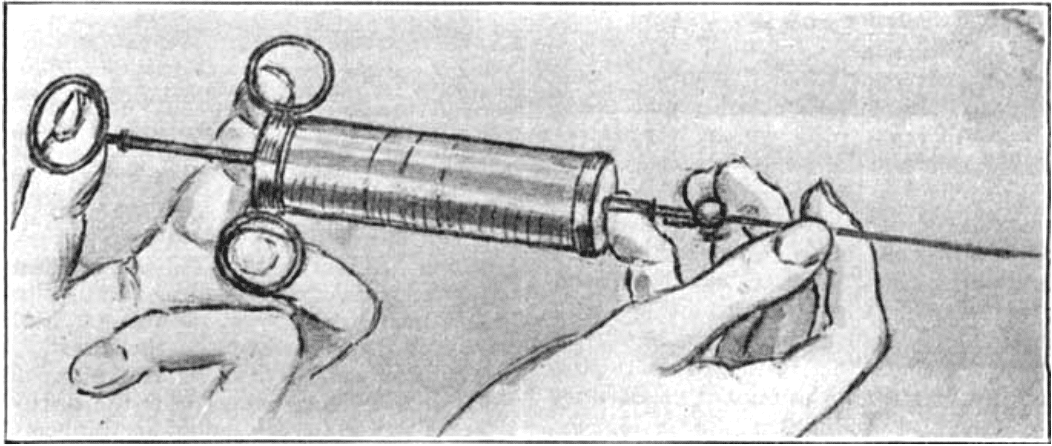
Dogliotti described his method of identifying the epidural space by the loss of resistance encountered as the needle passes through the ligamentum flavum into the epidural space. By applying constant pressure to the syringe plunger during needle advancement, the sudden decrease in resistance provided a reliable physiological sign of correct needle placement. This simple but powerful concept dramatically improved the safety, accuracy, and reproducibility of epidural anaesthesia.
Quando la punta dell’ago supera i legamenti gialli l’iniezione non incontra più alcuna resistenza e dà l’impressione di versarsi nel vuoto.
Dogliotti 1931
In his 1933 English-language synthesis, he reiterated the use of the simple tactile sign
As soon as the needle pierces the ligaments and arrives in the peridural space, all resistance is at once removed and the liquid enters with every facility
Dogliotti 1933
Through anatomical dissection, cadaveric injection studies, radiological imaging, and clinical observation, Dogliotti demonstrated that epidural anaesthesia acts primarily on the spinal nerves and ganglia extradurally, with “only a very small quantity” of anaesthetic passing into the cerebrospinal fluid. His contributions assisted in the transition of epidural anaesthesia from experimental innovation to standard clinical practice.
Cardiac surgery and extracorporeal circulation
From the late 1940s, Dogliotti emerged as a pioneer of cardiothoracic and cardiovascular surgery in Italy. At the University of Turin he established a surgical programme that combined experimental physiology with clinical innovation, particularly in situations of acute cardiopulmonary failure. Unlike many contemporaries pursuing complete cardiac replacement, Dogliotti conceptualised extracorporeal circulation primarily as a form of temporary circulatory assistance, analogous to assisted ventilation rather than total organ substitution.
August 7, 1951 – Dogliotti and Antonio Costantini performed the first documented successful human use of an apparatus for extracorporeal blood circulation. The patient was a 57-year-old man from Turin undergoing thoracotomy for a large mediastinal connective-tissue tumour causing severe compression of the great veins and right heart
After abrupt intraoperative deterioration (profound venous stasis, cyanosis, hypotension and impending cardiopulmonary arrest), they cannulated the left axillary vein (advancing a long cannula toward the superior vena cava) for venous drainage and returned oxygenated blood via the brachial artery, using systemic anticoagulation. Circulatory assistance was maintained for approximately 20 minutes, during which the patient stabilised sufficiently to allow tumour resection. Postoperatively, recovery was uncomplicated, with no biochemical or renal evidence of blood trauma.
Original
English
Appena iniziata la circolazione artificiale, rapidamente assistemmo ad un rialzo della pressione arteriosa che raggiunse i 110 mm di Hg… la stasi venosa e la cianosi si risolsero rapidamente… le condizioni del malato si stabilizzarono in modo così soddisfacente che ci fu consentita senza altri incidenti l’asportazione di gran parte della massa tumorale. La circolazione artificiale fu mantenuta per circa 20. Dogliotti 1951
As soon as artificial circulation was initiated, we rapidly observed a rise in arterial pressure to 110 mmHg… venous stasis and cyanosis resolved quickly… the patient’s condition stabilised so satisfactorily that removal of the greater part of the tumour could be completed without further incident. Artificial circulation was maintained for approximately 20 minutes. Dogliotti 1951
Dogliotti published this operation as proof that partial, time-limited extracorporeal circulation could be lifesaving in acute surgical crises. He proposed the term “circolazione assistita” (assisted circulation) and suggested future applications in pulmonary embolism, acute pulmonary oedema, asphyxia, and acute cardiac failure.
Pain therapy and Chemical Neurolysis
Dogliotti helped formalise pain therapy as a surgical and neuro-anatomical discipline. He pioneered and critically evaluated techniques of chemical neurolysis, including alcoholisation of posterior spinal roots, cranial ganglia, and peripheral nerves in patients with refractory neuralgia.
Through anatomical localisation, staged clinical series, and long-term follow-up, Dogliotti demonstrated that targeted interruption of pain pathways could provide lomg-lasting relief in conditions such as trigeminal neuralgia and essential facial spasm.
Major Publications
- Dogliotti AM. Proposta Di Un Nuovo Metodo Di Cura Delle Algie Periferiche – L’alcoolizzazione Sottomeningea Delle Radici Posteriori. 1931
- Dogliotti AM. Sulla Possibilità Di Lateralizzare E Rafforzare La Rachianestesia Mediante Aggiunta Di Alcool Etilico 1931
- Dogliotti AM. Esame Critico Della Tecnica E Dei Risultati Dell’alcoolizzazione Del Ganglio Di Gasser Per La Cura Della Nevralgia Ribelle Del Trigemino,in Base Ai 64 Casi Finora Da Me Trattati 1931 [chemical neurolysis]
- Dogliotti AM. Curriculum Ed Elenco Riassunto Delle Pubblicazioni Del Dr. Achille Mario Dogliotti. 1931
- Dogliotti AM. Un Promettente Metodo Di Anestesia Tronculare In Studio La Rachianestesia Peridurale Segmentaria 1931 [Dogliotti’s principle]
- Dogliotti AM. Research and clinical observations on spinal anesthesia: with special reference to the peridural technique . Anesthesia & Analgesia. 1933; 12(2): 59–65 [Dogliotti’s principle]
- Dogliotti AM. Sul Trattamento Dello Spasmo Facciale Essenziale. 1933
- Dogliotti AM, Costantini A. Primo caso di applicazione all’uomo di un apparecchio di circolazione sanguigna extracorporea [First case of the human use of an apparatus for extracorporeal blood circulation]. Minerva Chir. 1951 Nov 15;6(22):657-9.
References
Biography
- Un giorno col personaggio: Achille Mario Dogliotti. Incontri al microfono di Sergio Zavoli. RaiTeche
- Caldarola L. Prof. Achille Mario Dogliotti [Professor Achille Mario Dogliotti]. Cancro. 1965;18(5):403-5.
- Oliaro T. Ricordo di Achille Mario Dogliotti 25 Settembre 1897–2 Giugno 1966 [In memory of Achille Mario Dogliotti, 25 September 1897-2 June 1966]. Minerva Med. 1966 Oct 20;57(84):3487-8.
- Agostoni G. Achille Mario Dogliotti (Torino, 1897-1966) [Achille Mario Dogliotti (Turin, 1897-1966)]. Cardiol Prat. 1966 Apr;17(2):111-7.
- Borgno M. A ricordo di Achille Mario Dogliotti [In memoriam Achille Mario Dogliotti]. Minerva Urol. 1966 May-Jun;18(3):15.
- De Simone M. Ricordo del Prof. Achille Mario Dogliotti [A recollection concerning Professor Achille Mario Dogliotti]. Minerva Chir. 1966 Jun 30;21(12):564-5
- Kapronczay K. Achille Mario Dogliotti [Achille Mario Dogliotti]. Orv Hetil. 1978 Feb 5;119(6):343-4.
- Morino F. Achille Mario Dogliotti. Ann. Ital. Chir 1995;66(2): 295-296
- Моргошия Т.Ш. Акилле Марио Дольотти: к 120-летию со дня рождения. Анналы хирургической гепатологии. 2018;23(4):126-130.
Eponymous terms
- Ikle A. Preliminary report of new technique for epidural anaesthesia. Br J Anaesth. 1950 Jul;22(3):150-5.
- Vercellone A, Angelino PF, Linari F, et al. Il rene artificiale Dogliotti-Battezzati-Taddei nell’applicazione clinica [Clinical use of the Dogliotti-Battezzati-Taddei artificial kidney]. Minerva Nefrol. 1957 Apr-Jun;4(2):53-8.
- Naulty JS, Ostheimer GW, Datta S, Knapp R, Weiss JB. Incidence of venous air embolism during epidural catheter insertion. Anesthesiology. 1982 Nov;57(5):410-2.
- Simopoulos T, Peeters-Asdourian C. Pneumocephalus after cervical epidural steroid injection. Anesth Analg. 2001 Jun;92(6):1576-7.
- Wilson MJ. Epidural endeavour and the pressure principle. Anaesthesia. 2007 Apr;62(4):319-22.
- Waurick K, Waurick R. Epiduralanästhesie – Geschichte und Technik der Epiduralanästhesie [History and Technique of Epidural Anaesthesia]. Anasthesiol Intensivmed Notfallmed Schmerzther. 2015 Jul;50(7-8):476-82; quiz 483.
Eponym
the person behind the name

DM (UWA), BM (Indiana), FMusA, LMusA. Resident Medical Officer, Sir Charles Gairdner Hospital. Basic Surgical Streaming Program. Professional violinist, now aspiring surgeon. Loves music, opera, and operating.
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |