
![]()
Cannon Balls
aka Oncological Quandary 003
A 26 year-old male, with no previous history of seizures, was BIBA in status epilepticus. He was intubated for seizure management with propofol and clonazepam infusions.
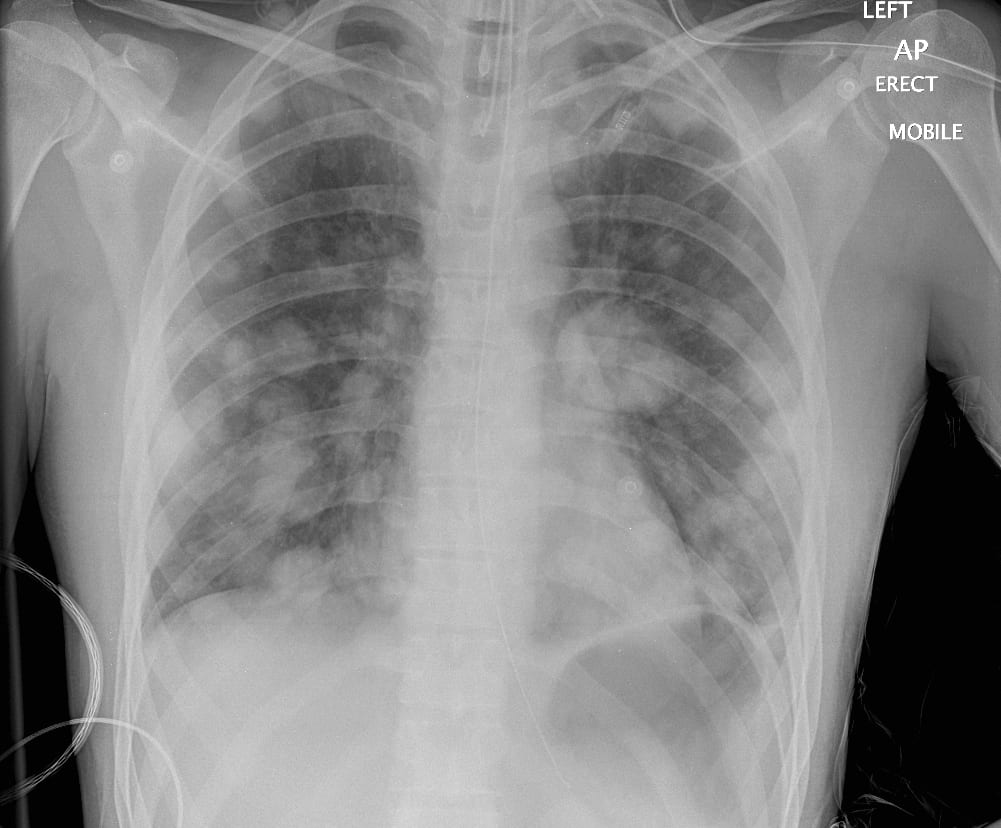
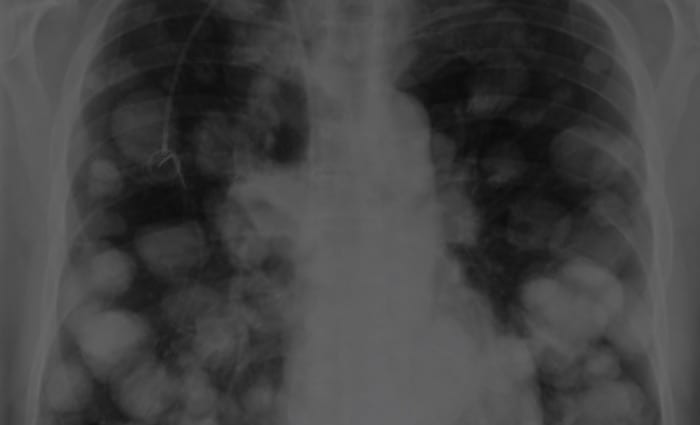
A chest XR was performed:
Questions
Q1. Describe and interpret the above chest x-ray.
Answer and interpretation
Cannon Ball lesions:
- The chest radiograph shows ‘cannon ball‘ lesions – multiple bilateral spherical lesions of varying size that are predominantly preipherally located.
- An endotracheal tube and nasogastric tube are present and appropriately positioned.
- The likely diagnosis is metastatic cancer involving the lungs.
But where is the primary?
- Tumors with rich systemic venous drainage are most likely to metastasize to the lungs.
- Choriocarcinomas, melanomas, testicular germ cell tumours, renal cancers, osteosarcomas and thyroid carcinomas.
- However, lung metastases most commonly arise from more common tumours.
- Breast, colorectal, prostate, bronchial, head/neck, and renal cancers.
Q2. What should be specifically looked for on clinical examination?
Answer and interpretation
The following should be carefully examined in a patient with suspected malignancy:
- all lymph nodes draining the region of a suspected lesion
- all remaining accessible lymph node groups
- the abdomen, specifically looking for hepato/splenomegaly and ascites
- the testes
- rectum
- lungs
- breasts and pelvis in females
- skin, nails and retina for melanoma
- focal neurological deficits
A large right-sided firm scrotal mass was palpable on physical examination and an urgent urology referral was made.
Ultrasonography confirmed the mass to be intratesticular with normal surrounding tissues. The mass was solid, ~6 cm in diameter, and had some cystic changes and slightly increased vascularity.
A CT head and chest were also performed, followed by an MRI of the brain, abdomen and pelvis once the patient was extubated. Sample images from the CT chest and MRI brain demonstrating the presence of lung and cerebral metastases are shown below:
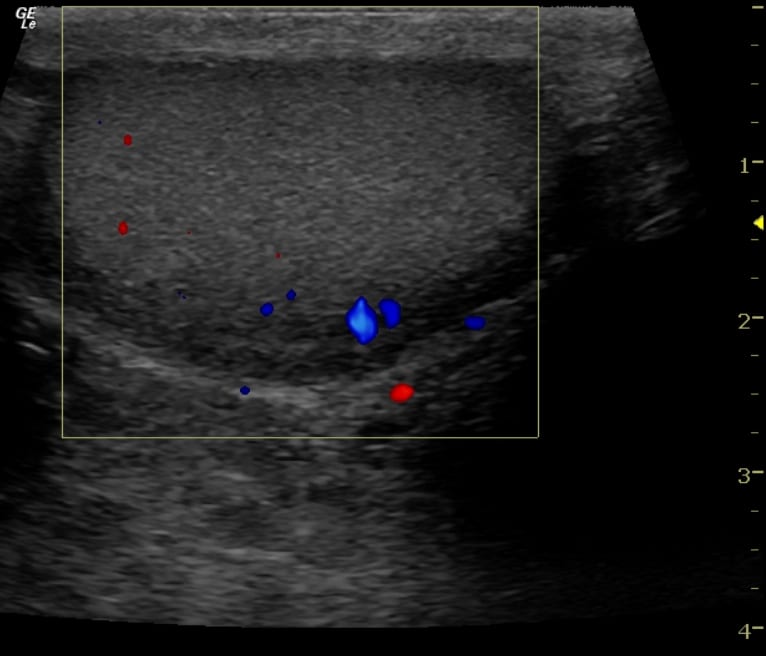
Sagittal view of normal testis 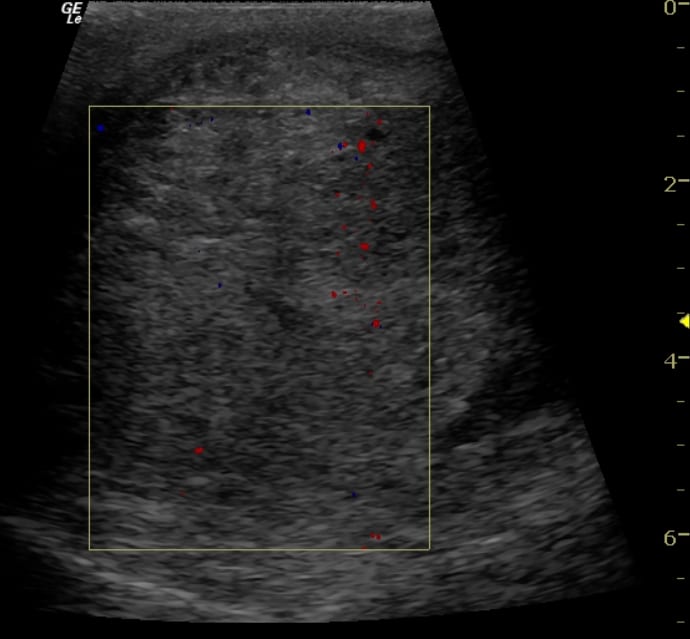
Sagittal view of abnormal testis 
CT Chest lung metastases 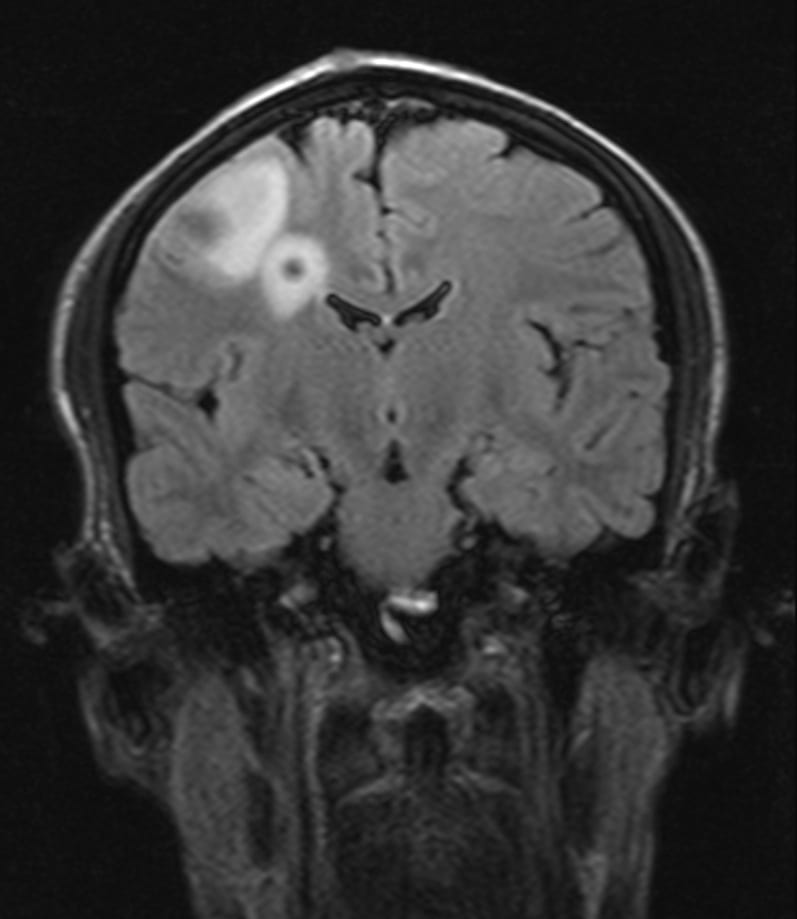
MRI brain metastases
Q3. Based on the findings in Q3 what is the likely diagnosis?
Answer and interpretation
Metastatic testicular cancer.
- Testicular cancer is the most commonly diagnosed cancer in men between the ages of 15 years and 35 years.
- About 1 in 20 testicular cancers have already metastasised at the time of diagnosis, and a similar number involve both testes.
- Risk factors include:
cryptorchidism, family history (especially first degree relatives), genetic disorders (e.g. Klinefelters and Down syndrome), infertility, testicular atrophy, HIV, white race and smoking.
There are numerous different types of testicular cancer. 95% are germ cell tumours (GCTs) and 1 in 3 of these are mixed cell types. Of the pure GCTs the main distinction is between:
- seminomas (~50%)
- non-seminoma germ cell tumours(NSGCT):
- including embryonal carcinomas, yolk sac tumours, teratomas, and choriocarcinomas
- mixed cell type tumours behave like NSGCTs.
- These are more aggressive than seminomas.
This patient was diagnosed with a NSGCT as both beta-human chorionic gonadotrophin (bHCG) (>350,000 mIU/mL) and alpha-fetoprotein (AFP) were grossly elevated.
- AFP is not elevated in pure seminomas.
The patient underwent a unilateral orchidectomy and BEP chemotherapy (bleomycin, etoposide and cisplatin) was commenced. He may also need radiotherapy and/or surgery to treat his cerebral metastases.
Q4. What toxicities due to the chemotherapy (mentioned in Q3) may occur?
Answer and interpretation
The major immediate toxicities associated with administration of BEP chemotherapy are:
- fatigue (39%)
- mucositis (25%)
- sensory neuropathy (20%)
- acute pulmonary toxicity (13%)
- ototoxicity (10%)
- hematologic toxicity (9%)
The components of BEP have different mechanisms of action and have different treatment toxicities:
- Bleomycin
- Inhibits DNA and to a lesser extent RNA synthesis, produces single and double strand breaks in DNA possibly by free radical formation.
- Toxicities:
- Pneumonitis that may lead to pulmonary fibrosis and death. Onset may be delayed up to 6 months. Risk is increased by use of supplemental oxygen, so minimal oxygen flow should be administered to maintain SaO2 ~88-92%.
- Chest pain and fever may be associated with administration. Myelosuppression is generally mild. Gastrointestinal symptoms, rashes and mucositis may occur.
- Etoposide
- A podophyllotoxin that inhibits topoisomerase II resulting in DNA strand breaks and inhibition of cell division in the late S and G2 phases of the cell cycle.
- Toxicities:
- Myelosuppression, neuropathy, gastrointestinal symptoms, and rashes – including Stevens-Johnson syndrome.
- Cisplatin
- A platinum-based compound that is activated within the cell by displacement of chloride ions, leaving positively charged molecules which react with DNA. DNA replication, transcription and cell division are inhibited, ultimately inducing apoptosis. It is cell cycle nonspecific and other mechanisms may also be involved.
- Toxicities:
- Cardiovascular effects (delayed): hypertension, dyslipidemia, coronary artery disease, thromboembolic events and Raynaud phenomenon.
- Neuropathy, seizures and ototoxicity.
- Nephrotoxicity as well as hypomagnesemia, hypophosphatemia and hypokalemia.
- Myeolosuppression, gastrointestinal symptoms and rashes.
Secondary malignancies are the most common cause of death in testicular cancer survivors (leukemia and solid tumours) and infertility is common.
Q5. What is this patient’s prognosis?
Answer and interpretation
- Testicular cancer has 95% survival overall and about 80% survival in the presence of metastases.
- However, this patient falls into the category of “poor-prognosis NSGCT” given that his bHCG is >50,000 mIU/mL. His 5 year survival is probably <70%.
References
- Kaufman DS, Saksena MA, Young RH, Tabatabaei S. Case records of the Massachusetts General Hospital. Case 6-2007. A 28-year-old man with a mass in the testis. N Engl J Med. 2007 Feb 22;356(8):842-9. [PMID: 17314344]
- Kaufman MR. Short- and long-term complications of therapy for testicular cancer. Urol Clin North Am. 2007; 34(2): 259-68. [PMID: 17484931]
- Shaw J. Diagnosis and treatment of testicular cancer. Am Fam Physician. 2008; 77(4): 469-74. [PMID: 18326165]
CLINICAL CASES
Oncology Quandary
Intensivist in Wellington, New Zealand. Started out in ED, but now feels physically ill whenever he steps foot on the front line. Clinical researcher, kite-surfer | @DogICUma |