
![]()
Funtabulously Frivolous Friday Five 349
Just when you thought your brain could unwind on a Friday, you realise that it would rather be challenged with some good old fashioned medical trivia FFFF, introducing the Funtabulously Frivolous Friday Five 349
Question 1
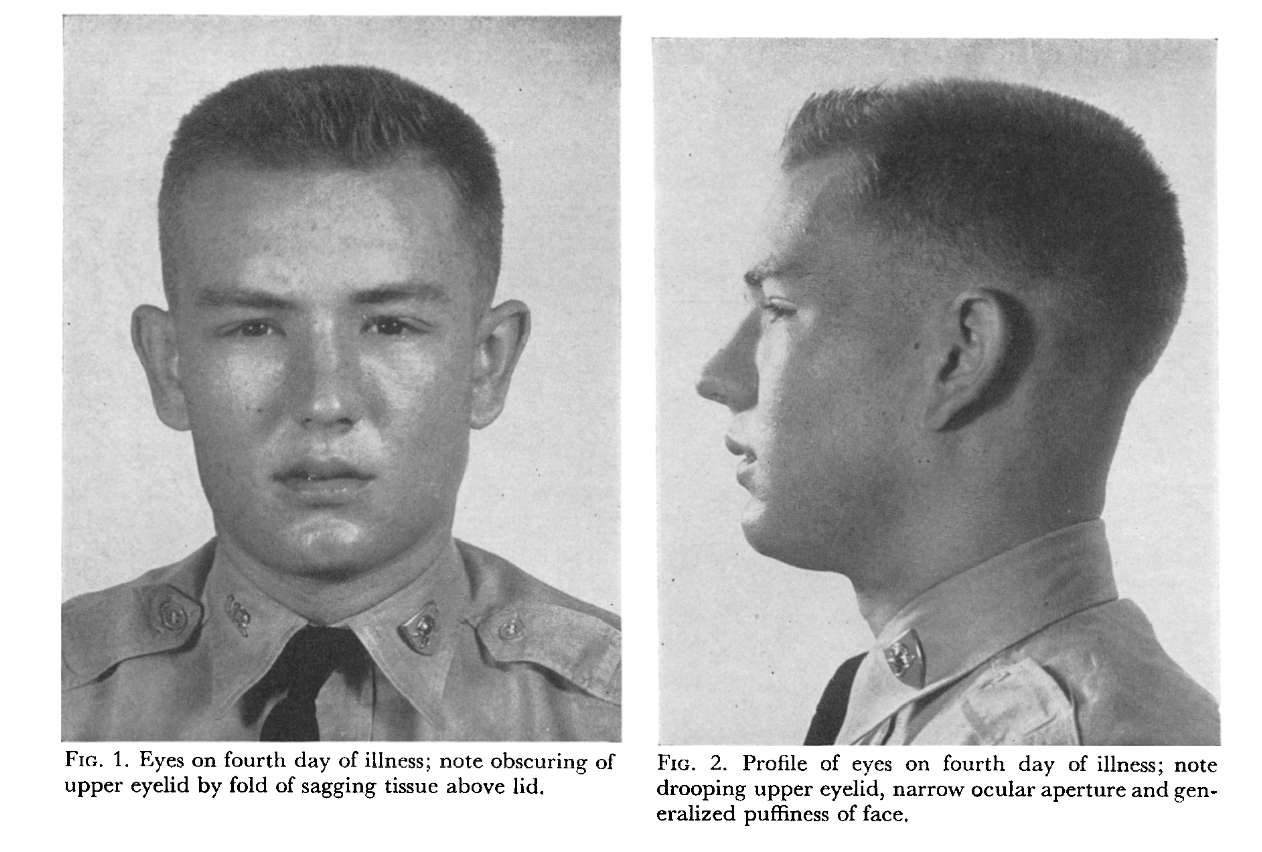
This young patient has bilateral supra-orbital swelling. What disease does the patient have? [Kudos to Dr Jeffery Eppler for sending the case]

Reveal the funtabulous answer
Infectious Mononucleosis.
The sign shown is Hoagland’s sign. Named after an American Colonel in 1952. He noted that nearly 50% of patients he saw with IM had periorbital oedema in the first five days of illness, and then it self-resolved. Potentially due to poor lymphatic drainage in the face. More recent studies have found that this periorbital oedema only occurs between 13-30% of the time. It is more common in children, women and with CMV rather than EBV.
Supra-ocular edema, present early in the course of illness, should be emphasized more as a helpful sign. It consists of a drooping of the swollen orbital portion of the upper eyelid upon the palpebral portion, and sagging of the latter, which is also swollen, resulting in a narrower ocular aperture.
Colonel Robert J Hoagland 1952
Reference:
- Hoagland RJ. Infectious mononucleosis. Am J Med 1952;13:158–71
- Esteban-Zubero E et al. Hoagland’s Sign: A Rare Initial Clinical Manifestation of Infectious Mononucleosis. Chronicle Journal of Clinical Case Reports. 2017;1[1]:005
Question 2
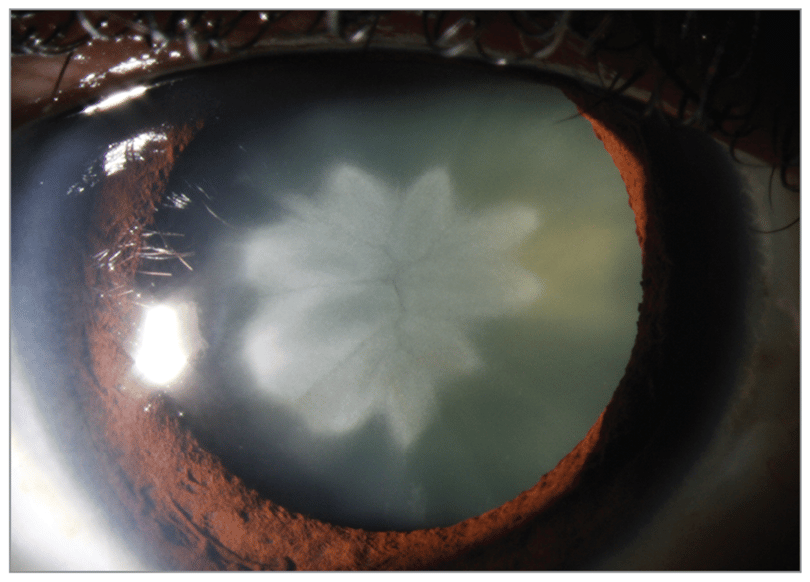
What happened to this patient?
Reveal the funtabulous answer
They were struck by lightning years ago.
The image shows a rosette-shaped cataract. This formed over years but can sometimes occur instantly and be more star-shaped. Usually bilateral, but there are case reports of unilateral cataracts on the side the patient was struck.
Reference:
- Venkateswaran N and Galor A. Rosette-Shaped Cataract Due to Lightning Injury. JAMA Ophthalmol. 2018;136(1):e175719. doi:10.1001/jamaophthalmol.2017.5719
Question 3
What single breath count result, could indicate a potential myasthenic crisis?
Reveal the funtabulous answer
Less than 25.
Single-breath count test (SBCT) can be helpful when the respiratory testing equipment is not available, or you are working in a remote centre or are doing telehealth.
An SBCT consists of making the patient count out loud after maximum inspiration. The result corresponds to the number reached with a normal voice without taking a breath. It is important to note that SBCT relates well to vital capacity in patients with neuromuscular diseases but can be more heterogenous in respiratory diseases, given a patient with COPD might have a prolonged expiratory phase compared to a patient with covid pneumonia compared to a patient with restrictive lung disease.
A new study carried out by an American team evaluated the SBC test carried out by telephone by a nurse trained in its use in 25 patients with generalized myasthenia gravis. Over a period of one year, they made 45 calls to their expert centre to report symptoms suggestive of a myasthenic crisis:
- An SBC test result below or equal to 25 had a positive predictive value of 71%, a sensitivity of 80% and a specificity of 60% to diagnose a myasthenic crisis;
- All the patients who could not count above 22 had an exacerbation of their disease, and none of the patients able to count above 28 had it;
- The most specific symptoms to predict an attack were, in this study, diplopia, dysphagia and ptosis.
As for other respiratory illnesses, SBCT scores below 21 usually indicate the need for some intervention in the literature to date. However, I think it has more utility as a simple way to track your patient’s progress and can be another clue that they are tiring and need additional support.
References:
- Escóssio AL et al. Accuracy of single-breath counting test to determine slow vital capacity in hospitalised patients. CEFAC 2019;21(2):e2119
- Kukulka K et al. A telephonic single breath count test for screening of exacerbations of myasthenia gravis: A pilot study. Muscle Nerve 2020;10.1002/mus.26987
- Longhitano et al. Single-Breath Counting Test Predicts Non-Invasive Respiraotry support Requirements in Patient with COVID-19 Pneumonia. J. Clin Med. 2022;11:179
- Quinn C et al. Single breath counting is an effective screening tool for forced vital capacity in ALS. ALS and FTD 2021;22(1)5-8
Question 4
Which laxative should you not give to children under the age of 5 due to skin sloathing and blisters?
Reveal the funtabulous answer
Senna
Don’t believe me, six poison centres in America over a 9-month period documented 111 unintentional senna ingestions in children five and under. Twenty-nine children (33%) experienced severe diaper rash. Ten children (11%) had blisters and skin sloughing. There was a significant increase in severe diaper rash (p < 0.05) and the onset of blisters and skin breakdown (p < 0.05) in children wearing diapers versus those who were fully toilet trained.
Reference:
- Spiller HA et al. Skin breakdown and blisters from senna-containing laxative in young children. Ann Pharmacother. 2003;37(5):636-9.
Question 5
Which pox virus is in the smallpox vaccine?
Reveal the funtabulous answer
Not cowpox, as you’ve always been told. It is vaccinia.
BS you cry; everyone knows Edward Jenner, a silver-haired surgeon made the discovery in 1976. Through some dubious ethics, he noticed beautiful milkmaids were never disfigured with smallpox scars nor died from the illness. He realised that those who had had the milder form of cowpox were immune to smallpox. He gets the wonderful idea of finding an eight-year-old boy, infecting him with cowpox (from a cow called blossom) and then exposing him to smallpox some weeks later. Fortunately, the boy survives, we have our first vaccine and interestingly, our first vaccine sceptics who produce claims children will grow horns and develop patches like milk cows.
To take a slight tangent it wasn’t Jenner who made this discovery of immunisation. John Fewster in Thornbury Gloucestershire had heard of an ancient method of rubbing small amounts of smallpox pus into an incision on healthy individuals. Unfortunately, 2-3% of people died from this method. He was, however, stunned when a smallpox scar never formed on a farmer. The farmer explained had recently been infected with cowpox. Fewster and Jenner were part of the same medical society and likely had discussed Fewster’s observations and this ancient concept of rubbing pus into wounds from Asia.
So, it all sounds like the vaccine used was from cowpox right? Advance a few years to 1939 and scientists test the vaccine for cowpox antibodies and discover it’s not cowpox.
There are many mammalian pox viruses including horsepox, camelpox, buffalopox, rabbitpox, mousepox and raccoonpox. Being immune to one usually gives you immunity to others hence why the reproduction of smallpox vaccine to protect humans against monkeypox.
So, if it’s not cowpox, what are we injecting? One theory was horsepox. Prior to Jenner scraping pus off what he thought was cowpox of a young maid milking blossom; an undergardener to the Earl of Berkeley had inadvertently transferred horsepox to his cattle. When said undergardener came to Jenner for his vaccine, it didn’t work despite multiple attempts. He never got a little scar from cowpox. Could this undergardner have actually transferred horsepox to cattle, or was he just immune because he had horsepox? Jenner relied on transferring pus from one human arm to another. When that chain broke, he had to look for an infected cow and in 1817 when that failed he switched to using horses. This worked so well he would transport infected equinated lymph nodes to spread his vaccines. Could this have been when the cowpox-based inoculation began to be replaced with one made from horsepox? Or was the virus always horsepox that had been transferred to cows?
An international team of scientists in 2017 found an old sample of a lymph vaccine kit and did a gene sequence. They didn’t find cowpox, but something related to horsepox. Other teams have had simar results, no one has ever found cowpox in these vaccine samples. So it looks like the majority of 19th and 20th Century vaccines were really horsepox. This means either cowpox was never used or the switch in vaccines happened rapidly.
But my answer said vaccinia, not horsepox. A final twist. In 1930 there was a radical shift in vaccines used. This shift is from horsepox to a mystery virus called vaccinia. No one knows the origin and it hasn’t been found in the wild. Remember I said that the original production line was pus from human arm to human arm. Then they decided to put the virus back into animals, either cows, horses, sheep or donkeys to increase production. As production stepped up globally, we suspect someone harvested what they thought was cow or horsepox from another farm animal. It was an unidentified imposter. It worked well, so no one noticed. The mystery virus became the dominant strain and in 1966 when the WHO announced the smallpox eradication campaign, it chose six vaccine strains, one of which was vaccinia. With each passing decade, vaccinia becomes more prominent and is now what we have left. Why no natural host? Horsepox has been eradicated in the wild due to smallpox vaccinations. If vaccinia is so effective, we’ve likely eradicated it from its natural host.
References
- BBC.com The mystery virus that protects against monkeypox. Accessed Nov 2022
… and finally, quotes:
You can’t do anything about the length of your life, but you can do something about its width and depth
John Ellison – 22.07.63 – 27.12.15

FFFF
Funtabulously Frivolous Friday Five
Dr Neil Long BMBS FACEM FRCEM FRCPC. Emergency Physician at Kelowna hospital, British Columbia. Loves the misery of alpine climbing and working in austere environments (namely tertiary trauma centres). Supporter of FOAMed, lifelong education and trying to find that elusive peak performance.
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |