
![]()
ICE 004: Chest pain ECG
A 64 year old man attends the ED after developing chest pain radiating to the jaw and right arm while playing tennis. The pain has now been present for nearly half an hour and continues unabated.
Questions:
- Describe his ECG
- What are the most important interventions for this man in ED?
- What is his likely subsequent treatment?
Reveal the ICE answer
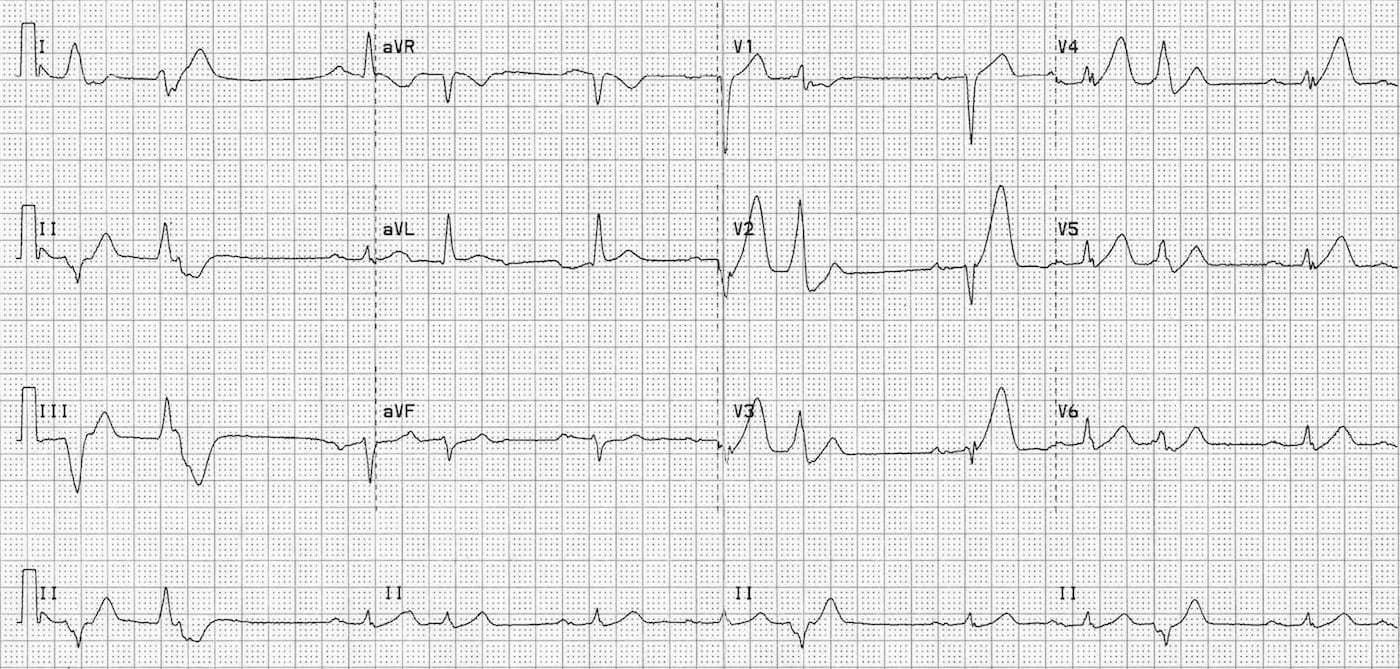
The ECG shows a number of changes suggesting acute myocardial ischaemia. There is sinus rhythm at 90 beats/minute with tall peaked T waves in leads V2-V4, but no ST elevation. There is additionally ST depression of 1mm in II, III and aVF (+/- V6) His axis is normal as are other intervals and morphology.
Although we classically look for ST elevation as the signifier of acute myocardial infarction, the earliest ECG change may be marked T wave peaking. We don’t see this often as it occurs so early in the infarct, typically the first 30 minutes. This patient later evolved marked ST elevation in V1-V4 diagnostic of an anteroseptal infarct from LAD occlusion.
The most important issue in this man is to recognise this as an acute coronary syndrome, and make sure he receives:
- Aspirin 300mg orally stat (antiplatelet action begins within 30 minutes)
- Heparin 5000U IV bolus and infusion
- Serial ECGs, initially every 15 mins, looking for ST elevation
IV GTN and morphine can be given to control his pain but they will have minimal effect on infarct size and mortality. Clopidogrel or Ticragelor may be indicated but in this case discuss with cardiology first.
He already meets criteria for coronary angiography. The only real question is the timing and urgency and this should be discussed as soon as possible with the interventional cardiologist. Should ST elevation develop on serial ECGs (as in this patient) then urgent transfer to the cath lab under a “Code STEMI” protocol is necessary

ICE CASES
Ian’s clinical emergencies
emergency physician keen on medical education and cycling