
![]()
Mallampati Score
The Mallampati Score is a grading system based on the visualisation of the pharyngeal structures during laryngoscopy.
A study of 210 patients confirmed the degree of difficulty in seeing three pharyngeal structures (uvula, soft palate and faucial pillars) as an accurate predictor of difficulty when using direct laryngoscopy.
A relatively simple grading system which involves preoperative ability to visualize the faucial pillars, soft palate and base of uvula was designed as a means of predicting the degree of difficulty in laryngeal exposure. The system was evaluated in 210 patients. The degree of difficulty in visualizing these three structures was an accurate predictor of difficulty with direct laryngoscopy (p < 0.001)
Mallampati SR et al, 1985
If the base of the tongue is disproportionately large relative to the capacity of the oropharynx, it would obscure the view of the faucial pillars, posterior part of the uvula and eventually the soft palate in that order. It would also render the angle to the trachea more acute and obscure the larynx – this anatomical relation was hypothesised by Mallampati and verified with his study published in 1985

History of the Mallampati Score
1975 – Seshagiri Rao Mallampati encountered a difficult tracheal intubation during a caesarean section. No harm came to the mother or the baby as a result but it was this event that led Mallampati down his route of inquiry into predicting difficult intubation which culminated in the development of the Mallampati score.
1983 – Letter to the editor in Canadian Anaesthetists’ Society Journal hypothesizing that preoperative airway assessment should be able to predict difficult intubation. The chief editor, Douglas Craig, wrote back to suggest he continued his work with a prospective study.
1985 – Mallampati published his scoring system.
Patients were divided into three classes:
- Class 1: Faucial pillars, soft palate and uvula could be visualized.
- Class 2: Faucial pillars and soft palate could be visualized, but uvula was masked by the base of the tongue.
- Class 3: Only soft palate could be visualized
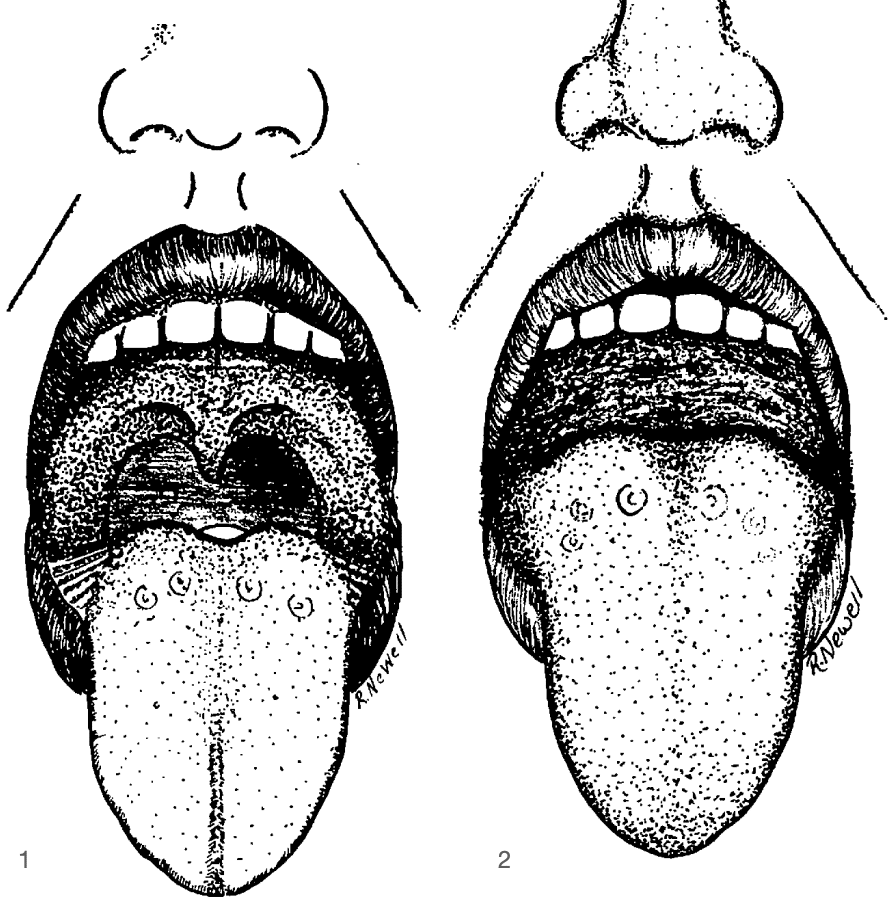
Fig 1. Grade I: Faucial pillars, soft palate and uvula are visible.
Fig 2. Grade III: None of the three pharyngeal structures are visible.
Mallampati SR et al, 1985
1987 – Samsoon and Young publish a new article to the Journal of Anaesthesia adding a 4th class to the Mallampati score
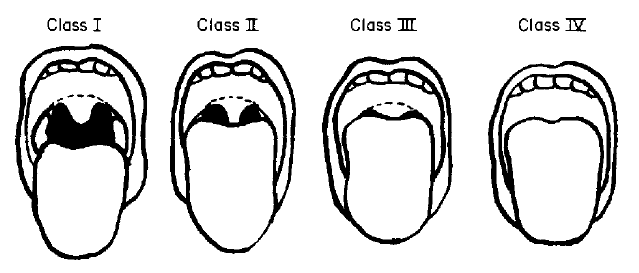
Pictorial classification of the pharyngeal structures as seen when conducting the tests. modified from Mallampati et al,
Note: Class III. soft palate visible; Class IV. soft palate not visible.
Samsoon GLT, Young JRB, Anaesthesia 1987
Associated Persons
References
- Mallampati SR. Clinical sign to predict difficult tracheal intubation (hypothesis). Can Anaesth Soc J. 1983 May;30(3 Pt 1):316-7.
- Mallampati SR, Gatt SP, Gugino LD, Desai SP, Waraksa B, Freiberger D, Liu PL. A clinical sign to predict difficult tracheal intubation: a prospective study. Can Anaesth Soc J. 1985 Jul;32(4):429-34.
- Samsoon GLT, Young JRB. Difficult tracheal intubation: a retrospective study, Anaesthesia 1987; 42: 487
- Tham EJ et al. Effects of posture, phonation and observer on Mallampati classification. Br J Anaesth. 1992 Jan;68(1):32-8.
- Myers KA, Mrkobrada M, Simel DL. Does this patient have obstructive sleep apnea?: The Rational Clinical Examination systematic review. JAMA. 2013 Aug 21;310(7):731-41
eponymictionary
the names behind the name

Bachelor of Medical Studies (BMedSt), Doctor of Medicine (MD) Bond University (Gold Coast). Emergency Medicine trainee who loves teaching, learning and improving the care of critically ill patients
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |