
![]()
ICE 013: Marathon runner develops chest pain
A 36 year old man has just completed a marathon. He develops chest heaviness, shortness of breath, nausea and feels dizzy and faint. He has no known past medical history and considers himself to be in excellent health, regularly competing in long distance running events.
His current basic observations are normal. This ECG was performed on his arrival in the ED.
Questions:
- What are the abnormal findings on his ECG?
- What conditions could explain the ECG findings?
- What further diagnostic tests are appropriate?
Reveal the ICE answer
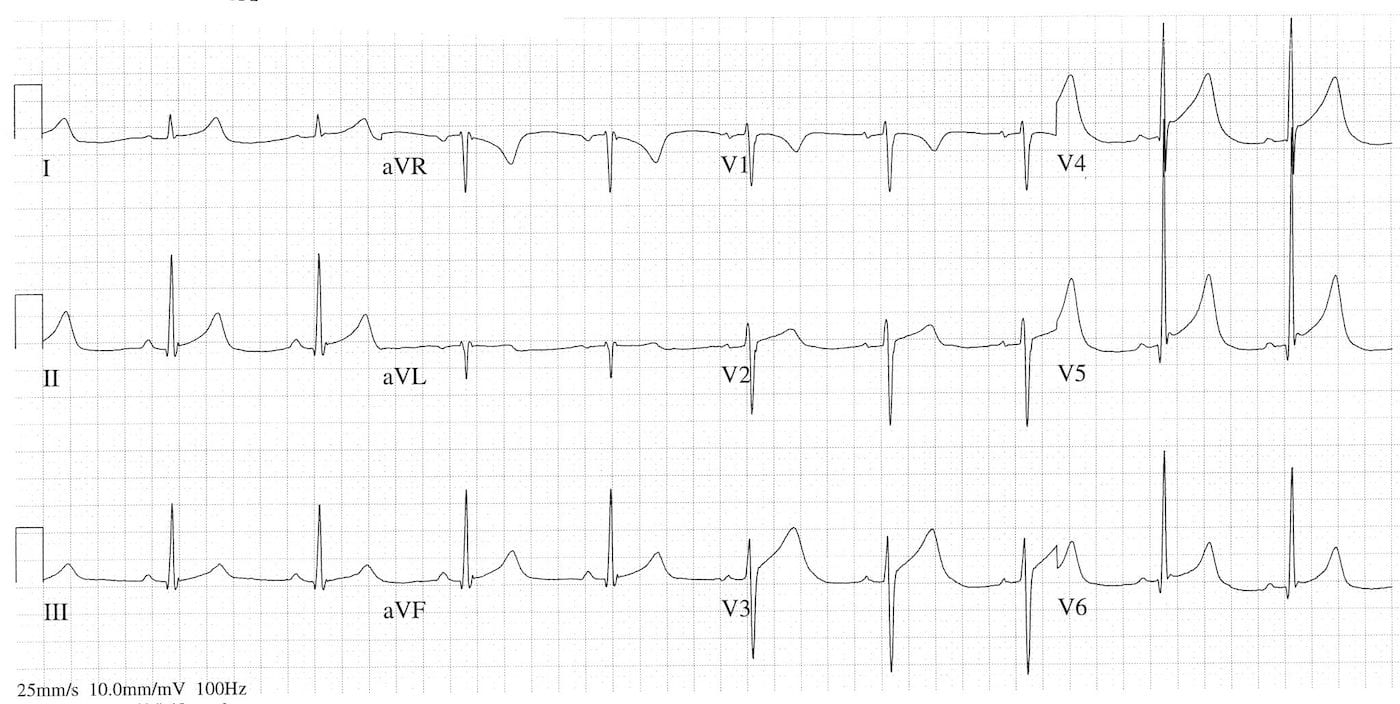
The ECG shows:
- Sinus bradycardia at 54 bpm
- PR interval 200 msec
- Elevated ST segments inferiorly and anteriorly with raised / notched J point
- Slightly concave upward ST segment morphology, except straight in V2
- Voltage criteria for LVH
- Prominent and peaked T waves especially in V2 – 6
These ECG findings could be consistent with acute anterolateral myocardial ischaemia and this needs to be the working diagnosis until proven otherwise. They could also be due to an as yet undiagnosed hypertrophic cardiomyopathy. The most probable cause however is so called “athletes heart”, a benign condition characterised by increased left ventricular muscle mass and cavity size due to athletic conditioning. As well as producing repolarisation abnormalities as seen on this ECG it can also produce bradycardia, first & second degree AV heart block, and RBBB .
Although a troponin would almost certainly be performed in this man it is unlikely to help initially as most endurance athletes have elevated troponins at race end. The most useful test would be an echocardiogram, as this will definitively diagnose hypertrophic cardiomyopathy and the wall motion abnormalities of acute ischaemia. It is particularly important to fully investigate such patients if they have QT prolongation on the ECG or a family history of cardiomyopathy or sudden premature cardiac death.
References:
- ECGpedia – ECGs in Athletes

ICE CASES
Ian’s clinical emergencies
emergency physician keen on medical education and cycling