
![]()
Merry Funtabulously Frivolous Friday Five 264
Just when you thought your brain could unwind on a Friday, you realise that it would rather be challenged with some good old fashioned medical trivia FFFF, introducing the Funtabulously Frivolous Friday Five 264 – Christmas Edition
Question 1
What condition would you expect to improve if you sustained a snowball to the eye?
Reveal the funtabulous answer
Myasthenia Gravis
Either edrophonium or an ice bag test can be used to diagnose Myasthenia Gravis.
Edrophonium is a short-acting acetylcholinesterase-blocking agent that will produce an increase in ACh in the synaptic cleft and thus a reduction in ptosis. Give 1-2mg IV as a test dose in case of a severe reaction followed by 3mg 1 min later and finally a 5mg dose.
This drug is the equivalent to organophosphate so have atropine on standby to resolve any secretions / bradycardia. Also probably not on Santa’s wish list for your department therefore…..
The ICE pack test: Myasthenia Gravis is exacerbated by heat therefore it should improve with ice. A pack of ice is applied on the affected eye for 2 minutes. An improvement in ptosis of at least 2mm is considered positive (pooled sensitivity 0.94% and specificity 0.97%). It will also improve the patients aim when firing the next snowball.
References:
- Liu WW, Chen A. Diagnosing Myasthenia Gravis with an Ice Pack. N Engl J Med. 2016 Nov 10;375(19):e39.
- Kearsey C, Fernando P, D’Costa D, Ferdinand P. The use of the ice pack test in myasthenia gravis JRSM Short Rep. 2010 Jun 30;1(1):14.
Question 2
What genetic condition gives the person Elf like facies?
Reveal the funtabulous answer
Williams Syndrome
Newborns with Williams syndrome have characteristic “elfin-like” facial features including an unusually small head (microcephaly), full cheeks, an abnormally broad forehead, puffiness around the eyes and lips, a depressed nasal bridge, broad nose, and/or an unusually wide and prominent open mouth.
In most individuals with Williams syndrome, the disorder appears to occur spontaneously for unknown reasons however, familial cases have also been reported. Sporadic and familial cases are thought to result from deletion of genetic material within a specific region of chromosome 7 (7q11.23).
There are about 20,000 babies born with Williams syndrome per year in the United States. Other abnormalities include:
- Supravalvular aortic stenosis (in 70 percent of cases),
- Renal artery stenosis
- Pulmonic valve stenosis
- Constipation / Diverticulosis
- Failure to Thrive
- Sensorineural hearing loss
- Idiopathic hypercalcemia
- Mild to moderate intellectual disability
Young patients with WBS tend to be very social, gregarious, and often overly friendly with strangers. See the video below for further details:
- Williams JC, Barratt-Boyes BG, Lowe JB. Supravalvular aortic stenosis. Circulation. 1961 Dec;24:1311-8.
Question 3
We all know how important it is to go to bed on Christmas Eve and not wake until the morning, but patients in the film ‘Awakenings’ didn’t wake for decades – imagine how many Christmas presents they finally had under the tree!
What medical condition did they have which resolved after taking L-DOPA?
Reveal the funtabulous answer
Encephalitis Lethargica
The film Awakenings is based on Oliver Sacks memoir of the same title and tells the story of Dr Malcolm Sayer who in 1969 discovered the benefits of L-DOPA in patients with Encephalitis Lethargica.
PLOT: Dr. Malcolm Sayer (Robin Williams) is a dedicated and caring physician at a local hospital in the The Bronx borough of New York City. After working extensively with the catatonic patients who survived the 1917–1928 epidemic of encephalitis lethargica, Sayer discovers certain stimuli will reach beyond the patients’ respective catatonic states; actions such as catching a ball, hearing familiar music, and experiencing human touch all have unique effects on particular patients and offer a glimpse into their worlds. Leonard Lowe (Robert De Niro) proves elusive in this regard, but Sayer soon discovers that Leonard is able to communicate with him by using an Ouija board.
After attending a lecture at a conference on the subject of the L-Dopa drug and its success with patients suffering from Parkinson’s disease, Sayer believes the drug may offer a breakthrough for his own group of patients. A trial run with Leonard yields astounding results: Leonard completely “awakens” from his catatonic state.
“They would be conscious and aware – yet not fully awake; they would sit motionless and speechless all day in their chairs, totally lacking energy, impetus, initiative, motive, appetite, affect or desire; they registered what went on about them without active attention, and with profound indifference. They neither conveyed nor felt the feeling of life; they were as insubstantial as ghosts, and as passive as zombies.”
Oliver Sachs – Awakenings p14.
Encephalitis Lethargica was first described in 1917 by the neurologist Constantin von Economo and the pathologist Jean-René Cruchet. The cause for the disease is uncertain.
Von Economo’s description of the 1916–1917 outbreak in Vienna was the first to delineate a constellation of signs and symptoms suggestive of a distinct disease entity. He identified 3 distinct clinical patterns of EL while emphasising that symptoms often overlapped and that even in the same patient, characteristics of each of the different patterns might prevail at different stages of the disease.
The somnolent-opthalmoplegic form of EL predominated during the 1916–1917 outbreak in Vienna. It was characterized by a brief, nonspecific prodrome consisting of malaise, headache, and mild fever. Von Economo emphasized that the sudden high fever, myalgias, and upper respiratory symptoms characteristic of influenza were absent. The patient became increasingly somnolent until he fell into a deep sleep from which he could easily be roused, but into which he immediately relapsed when stimulation ceased. Somnolence usually lasted 1 or 2 weeks, after which it either worsened, resulting in coma leading to death, or gradually diminished until full recovery. The appearance of palsies during the first few days of the illness, especially of the external and internal eye muscles with resultant ptosis and diplopia, was a consistent characteristic. The extremities often became profoundly weak or hypotonic, but occasionally muscle groups developed rigidity. An expressionless, mask-like facies was frequently described. The descriptive epithet “sleepy sickness” was often attributed to this form of the disease. The mortality associated with this type of EL was approximately 50%, but chronic debility and neurologic sequelae were uncommon in this form of EL.
The hyperkinetic form of EL was characterized by restlessness as the dominant symptom, which assumed the form of motor disturbances including twitching or jerking of muscle groups or an anxious, even frenzied mental state. Onset was more sudden than in the somnolent form and often included severe back and neck pain, prostration, and weakness, followed by increasing mental and motor unrest. Insomnia or inversion of sleep patterns were common symptoms. Although this form of EL bore little resemblance to the somnolent variety, both included a profound disturbance of sleep patterns, reflecting localized damage in related functional areas of the brain. While diplopia and ptosis were uncommon in the hyperkinetic form, disturbances of the intra-ocular muscles were almost always present. As the disease progressed, involuntary movement increasingly interfered with voluntary actions, making the disease difficult to distinguish from chorea. Prognosis of the hyperkinetic form varied. Mortality in the initial stages was higher than in the somnolent-opthalmoplegic form, with sudden death occurring at any time.
Although the amyostatic-akinetic form of EL was the least common manifestation of acute EL, it was associated with a high proportion of chronic sequelae. In its chronic form, von Economo designated the disease as parkinsonism. The weakness and rigidity occasionally seen in somnolent EL became prominent symptoms in amyostatic-akinetic EL. The condition bore a striking resemblance to the bradykinetic component of the disease described by parkinson in 1817 as paralysis agitans, although concomitant tremor was unusual. These patients also exhibited sleep inversion and ophthalmoplegic disturbances, including diplopia, ptosis, and general weakness of the eye-muscles. Evolution of this form of EL into chronic parkinsonism was a recognized clinical entity as early as 1921.
- von Economo C. Encephalitis lethargica. Wiener klinische Wochenschrift. 1917;30:581–85 with full transcript in Die Encephalitis lethargica. 1918
- Pearce JM. Baron Constantin von Economo and encephalitis lethargica. J Neurol Neurosurg Psychiatry. 1996;60(2):167.
- Reid AH, McCall S, Henry JM, Taubenberger JK.. Experimenting on the Past: The Enigma of von Economo’s Encephalitis Lethargica. J Neuropathol Exp Neurol. 2001 Jul;60(7):663-70.
Question 4
In the Northern hemisphere the flu season is upon us, and while 50% of the population suffer more than the other half, is it fair to use such pejorative terms as ‘man flu’ and kick them back out to the waiting room?
Christmas BMJ 2017 explores the issue: Are men wimps? What is the latest theory for why men are so susceptible to the flu?
Reveal the funtabulous answer
Immunologically inferior.
The sex difference in immunity has been suggested to be modulated by hormonal differences, with oestradiol being immunoprotective and testosterone being immunosuppressive. Hormonal influence on immune response is supported by evidence that pregnant women have more severe influenza symptoms and reduced symptoms from autoimmune diseases than non-pregnant women.
The concept of man flu, as commonly defined, is potentially unjust. Men may not be exaggerating symptoms but have weaker immune responses to viral respiratory viruses, leading to greater morbidity and mortality than seen in women. There are benefits to energy conservation when ill. Lying on the couch, not getting out of bed, or receiving assistance with activities of daily living could also be evolutionarily behaviours that protect against predators. Perhaps now is the time for male friendly spaces, equipped with enormous televisions and reclining chairs, to be set up where men can recover from the debilitating effects of man flu in safety and comfort.
Reference: Sue K. The Science behind “man flu”. BMJ 2017;359:j5560
Question 5
Working at Christmas has its perks – no fighting over getting a car space for one but it’s often difficult to get hold of your on-call colleagues.
Which top 3 specialties will most likely be on the golf course this Christmas when you try to call them in?
Reveal the funtabulous answer
Vascular surgery (15.5), Neurology (15.2) and Dermatology (14.5) played the most games over a 6 month period.
Orthopaedic surgery (8.8%), Urology (8.1) and Plastic surgery (7.5%) have the highest percentage of golf players in their retrospective groups.
Vascular surgery (14.7), Thoracic surgery (14.8) and Orthopaedic surgery (14.9) have the best handicaps. Don’t bet against these physician groups.
Internal medicine had the lowest percentage of golfing physicians at 2.9%, Endocrinology had the worst handicap at 18.1 and haematology played the least amount of games in the past 6 months at 12.3.
Emergency medicine was fairly middle of the road with 4.4% of us playing, a handicap of 15 and getting in 13.5 games in the past 6 months.
All in all, physicians are bad at golf with non-physicians having a better handicap. Finally, the paper ponders the question, do patients receive inferior treatment after a subsequent bad day on the course? – more studies are required.
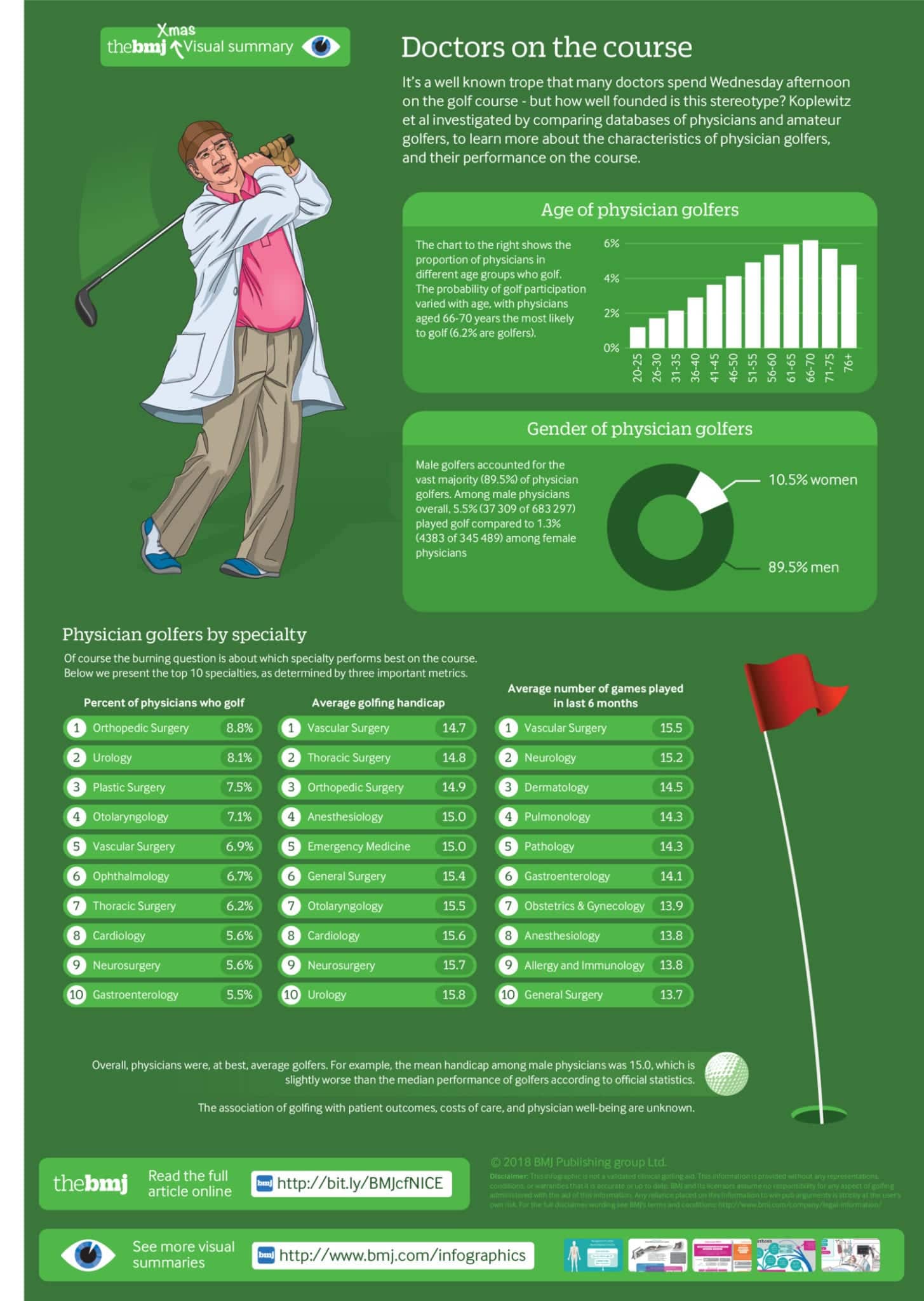
Reference: Koplewitz G et al. Golf habits among physicians and surgeons: observational cohort study. BMJ 2018;363
…and finally

FFFF
Funtabulously Frivolous Friday Five
Dr Neil Long BMBS FACEM FRCEM FRCPC. Emergency Physician at Kelowna hospital, British Columbia. Loves the misery of alpine climbing and working in austere environments (namely tertiary trauma centres). Supporter of FOAMed, lifelong education and trying to find that elusive peak performance.

Hi Neil, so thats where you went. Enjoy the FFFF, and to add that the co-author of the Williams paper was a Kiwi, though he may have enn overseas in 1961.
Great to hear from you Stu. Mike is looking into Williams – apparently he disappeared, its all a bit of a mystery. Miss you guys in CHCH.