
![]()
Pacemaker Panic #2
aka ECG Exigency 016
A 68-year old woman presents by ambulance to the Emergency Department. Per the ambulance crew, she was brought from home after experiencing 7 out of 10 chest discomfort and weakness. She has a history of hypertension that is well controlled with furosemide, and has a pacemaker because her “heart used to go funny.”
The ambulance crew are basic life support only, so the patient has received 324mg of aspirin, and oxygen by nasal cannula. Upon arrival she is seated upright on the stretcher breathing rapidly, with the following vitals: heart rate 107, blood pressure 180/110, respiratory rate 20 and slightly labored, oxygen saturation 100% on 2 L/min by nasal cannula, and blood glucose 110 mg/dL (6.1 mmol/L).
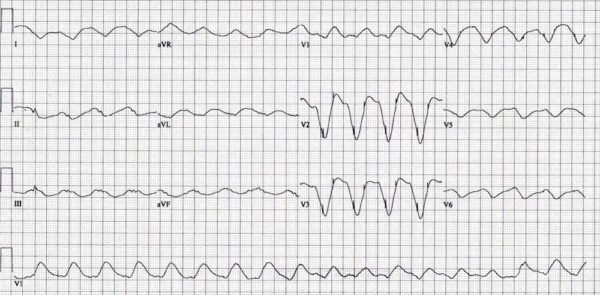
The medical student said the patient appeared to be in ventricular tachycardia on the monitor, and so has brought the crash cart to the bedside. Her ECG is shown below:
Questions
Q1. Describe the ECG
- Broad complex tachycardia at 107 bpm.
- Extremely wide QRS complexes.
- Indeterminate QRS axis.
- Pacemaker spikes dissociated from QRS complexes.
Q2. What is the significance of these ECG findings?
here are a number of causes for a wide QRS complex, including:
- Bundle branch block
- Pacemaker
- Wolff-Parkinson-White syndrome
- Ventricular Rhythm
- Metabolic
- Sodium Channel Blockade
- Nonspecific Intraventricular Conduction Delay
However, when the QRS duration is greater than 200 ms, hyperkalemia should immediately move to the top of the differential. Hyperkalemia would also explain the pacemaker failure to capture. When the QRS becomes too wide, the pacemaker attempts to trigger during the refractory period and fails to capture.
Q3. What other diagnostics are warranted at this point?
- The ECG alone is neither particularly sensitive nor specific for diagnosing hyperkalemia.
- Serial blood draws should be used to track the patient’s potassium.
- A VBG using an ED-based gas analyser is often the most rapid way to get an initial potassium reading, and may give useful information about acid-base status.
- Urea and electrolytes should be checked to detect renal dysfunction.
- Her initial potassium is 8 mmol/L.
Q4. How would you manage this patient?
There are 3 goals in treating hyperkalemia: membrane stabilisation, shift potassium into cells, and increased potassium elimination from the body.
Membrane stabilisation
- Calcium chloride and gluconate are both effective. Remember that calcium gluconate does not have to be metabolised by the liver to work.
Shift potassium
- Sodium bicarbonate: alone does not lower potassium, and there is debate whether it will potentiate the effects of salbutamol / albuterol and insulin + dextrose.
- Insulin + Dextrose
- Salbutamol / Albuterol
Increase potassium elimination
- Diuretics such as furosemide
- Dialysis
- Kayexalate: while a mainstay of treatment, there is no evidence that kayexelate reduces potassium levels. The original research that promoted its has serious methodological flaws.
After your initial round of treatment, you acquire another ECG
Show ECG
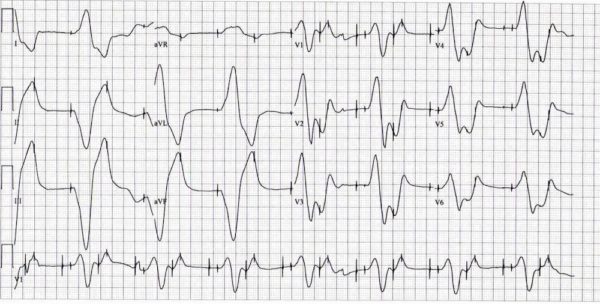
Q6. Can you describe this ECG?
- Underlying rhythm is a dual chamber AV sequential pacemaker.
- Pacemaker rate: 100 bpm, Ventricular rate captured: 50 bpm.
- Pacemaker failure to capture
- Wide QRS complex
- ST-T wave abnormalities
Q7. What are the significance of these ECG findings?
- While the patient’s pacemaker has taken over, it is still unable to capture 100% of the time.
- The wide QRS from the underlying hyperkalemia is causing half the pacemaking impulses to fall during the refractory period of the QRS and fail to conduct.
Q8. Based on the ECG findings, do you believe the patient’s condition has improved?
- Yes.
- A blood draw confirms that the patient’s potassium level has dropped to 6.6 mmol/L.
Q9. Can you guess how the patient wound up in this state?
- Furosemide is a loop diuretic that when administered alone may cause low potassium levels.
- As such, many patients on furosemide will be taking a potassium supplement.
- After additional interviewing, you find that the patient misunderstood the dosing instructions for the potassium and unintentionally overdosed.
References
- Martin TJ, Kang Y, Robertson KM, Virji MA, Marquez JM. Ionization and hemodynamic effects of calcium chloride and calcium gluconate in the absence of hepatic function. Anesthesiology. 1990 Jul;73(1):62-5.
- Wrenn KD, Slovis CM, Slovis BS. The ability of physicians to predict hyperkalemia from the ECG. Ann Emerg Med. 1991 Nov;20(11):1229-32.
- Montague BT, Ouellette JR, Buller GK. Retrospective review of the frequency of ECG changes in hyperkalemia. Clin J Am Soc Nephrol. 2008 Mar;3(2):324-30.

CLINICAL CASES
ECG Exigency
Emergency Physician in Prehospital and Retrieval Medicine in Sydney, Australia. He has a passion for ECG interpretation and medical education | ECG Library |
ECG2:
DDD 50 beat per min(right apex pacing)
Atrial pacing and Perception dysfunction
would you like to contact me on Twitter?
Just as a feedback, Calcium chloride is the one without liver metabolism, that’s why it is used in codes. Gluconate does need liver metabolism but it is less corrosive and easier to use, hence the use of it in stable patients. I hope this helps. Thank you for all that you do!
Hi Isaac,
Thanks for commenting! When administered, the calcium ions are available immediately after injection without requiring metabolism through the liver. Interestingly gluconate isn’t a very effective bicarbonate precursor, and while it IS hepatically metabolised, apparently only about 10-40% actually does get metabolised, and the rest is excreted unchanged in the urine. The reason for use of calcium chloride in code blues is due to potency. Where 1g of calcium chloride (our standard solution in Australia, in 10mL of a 1% solution) contains 6.8mmol of calcium ions, and 1g of calcium gluconate (again, standard in 10mL of a 1% solution) contains 2.2mmol of calcium ions. In code blues where a patient is in a low or no flow state, you want as many of those ions getting to those cardiac myocytes as possible…
We also frequently use calcium chloride in patients who are critically unwell, and where we need to administer higher doses of calcium ions… ideally this is done via central access as, you are quite right, it is a venoirritant.
Thanks,
James