
![]()
Pain free and in VT?
aka ECG Exigency 002
Can you take a look at the patient in bed 2? I think he’s having runs of VT!
You are called to the monitored area in ED to see a 62-year man who is awaiting a bed under the medics for investigation of an episode of chest pain earlier in the day. He is currently pain free, sat up in bed looking undistressed with a blood pressure of 150/90.
The monitor shows intermittent runs of a broad complex rhythm. His ECG is shown:

Questions
Q1. Describe the ECG
e ECG shows sinus rhythm with rate-dependent left bundle-branch block.
The first eight QRS complexes show:
- Sinus rhythm at around 82 bpm
- Normal PR interval (160ms)
- Broad complexes (120ms)
- Typical LBBB morphology (leftward axis, deep S-wave in V1, broad ‘M’ pattern in I, aVL)
The remainder of the ECG shows:
- Slowing of the sinus rate to 60bpm
- Narrowing of the QRS complexes to 80ms
- Disappearance of the LBBB pattern
The appearance in the chest leads is suggestive of Wellens syndrome, with:
- Deep T wave inversions in the right- and mid-precordial leads (V1-4)
- Biphasic T wave morphology in V2
There is also subtle T wave flattening and ST depression in the last four complexes of the lead II rhythm strip, indicating possible inferior ischaemia.
Q2. What is the electrophysiological basis for the broad complex rhythm?
Rate-dependent bundle-branch block (AKA “tachycardia-dependent BBB”) is simple to understand:
- One of the bundle branches becomes diseased and rather than fail completely (which would produce a fixed bundle branch block pattern), it develops a prolonged refractory period.
- Below a certain rate, this prolonged refractory period has no effect; impulses are conducted normally.
- Above the ‘critical’ rate, the diseased bundle branch is unable to conduct impulses fast enough and a bundle branch pattern appears on the ECG.
- Rate related fascicular blocks (LAFB, LPFB) may also occur, producing left or right axis deviation respectively when the rate increases above a certain threshold.
Bradycardia-dependent bundle branch block (which is much less common) is essentially the opposite:
- A bundle branch pattern appears whenever the rate falls below a certain rate.
- This happens because of a tendency for damaged cells within the bundle branches to leak their charge and become inexcitable when the intervals between impulses are too long.
Q3. What treatment is required for the broad complex rhythm?
No specific treatment is required for rate-dependent LBBB.
Q4. What is the clinical significance of the other ECG changes?
In a patient presenting with recent chest pain, an ECG showing biphasic or deeply inverted T waves in leads V1-4 is highly specific for a critical occlusion of the proximal LAD – Wellens Syndrome
These patients may be pain free by the time the ECG is taken and have normally or minimally elevated cardiac enzymes; however, they are at extremely high risk for extensive anterior wall MI within the next 2-3 weeks.
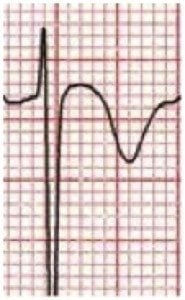
There are two types of T wave inversions seen in Wellens syndrome.
Type A T-waves are biphasic:
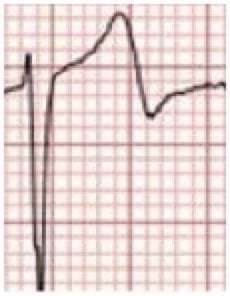
Type B T-waves are deeply, symmetrically inverted:
Q5. How should this patient be managed?
- This patient needs urgent cardiology referral, admission to a monitored bed and early PCI (ideally within 48 hours).
- Medical management (including thrombolysis) is frequently ineffective in this condition.
- The only way to prevent progression to extensive anterior MI is revascularization via PCI or CABG.
References
de Zwaan C, Bär FW, Wellens HJ. Characteristic electrocardiographic pattern indicating a critical stenosis high in left anterior descending coronary artery in patients admitted because of impending myocardial infarction. Am Heart J. 1982 Apr;103(4 Pt 2):730-6.

CLINICAL CASES
ECG Exigency
Emergency Physician in Prehospital and Retrieval Medicine in Sydney, Australia. He has a passion for ECG interpretation and medical education | ECG Library |
Could this inverted T wave be a chatterjee effect ?
You’ve written that the first ECG is left axis? It looks like normal exist to me with leads 1 and 2 positive and lead aVf negative?
ECG 1 shows normal axis doesn’t it???