
![]()
Scimitar Syndrome
Description
The scimitar syndrome is a complex malformation of the heart, lungs, and blood vessels. The main feature of this malformation is the anomalous drainage of the pulmonary veins into the inferior vena cava.
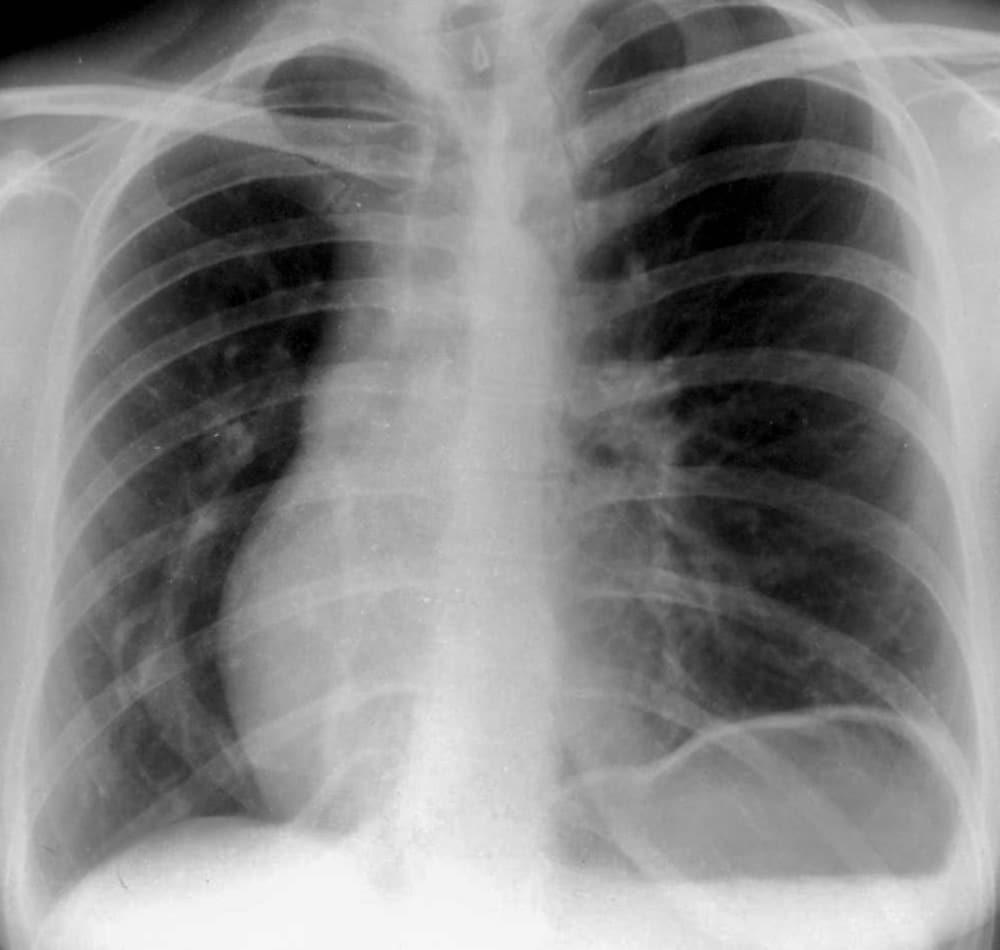
Scimitar syndrome represents a combination of pulmonary hypoplasia and partial anomalous pulmonary venous return (PAPVR) which can be noted on CXR and can be documented angiographically. Classically, there is displacement of the cardiac silhouette to the right; a small right lung; with a prominent curved (‘scimitar’) vein draining the right lung to the inferior vena cava (IVC). The majority of cases are manifest on the right side.
- Scimitar: The English word scimitar refers to a single-edged backsword or sabre with a curved blade. Probably adapted from the Italian word scimitarra in the 16th century. The term was used for all curved ‘Oriental’ blades as distinct from the straight, double-edged European swords of the time.
- Pulmonary hypoplasia (PH): deficient or incomplete development of parts of the lung.
- Partial anomalous pulmonary venous return (PAPVR): rare congenital cardiovascular condition in which some of the pulmonary veins, but not all, drain into the systemic circulation rather than in the left atrium. [aka partial anomalous pulmonary venous connection (PAPVC)]
History
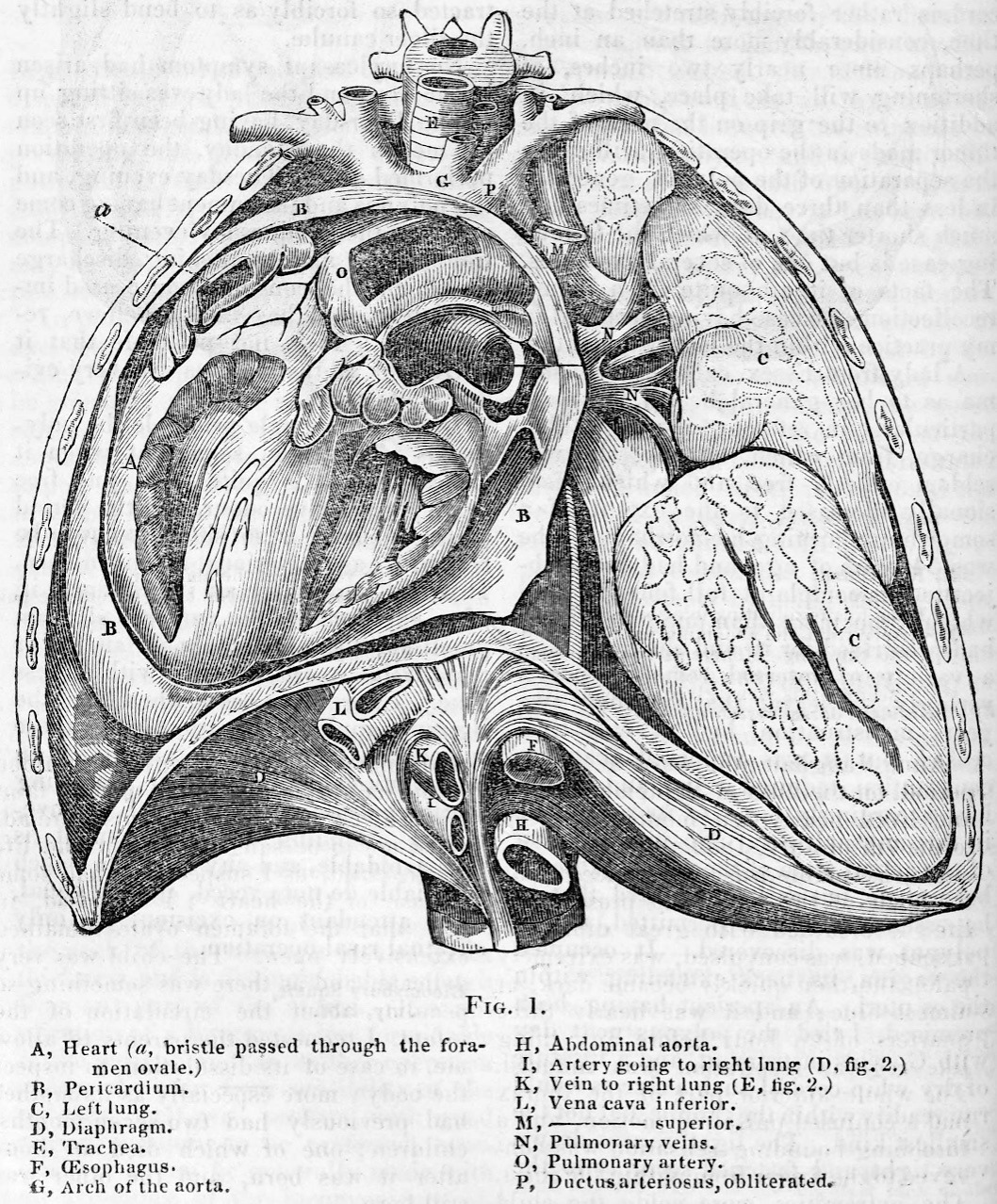
1836 – English pathologist George Cooper published an “account of a case which fell under my own notice, of transposition of the heart, and imperfect development of the right lung, while the vessels and viscera of the abdomen retained their usual relative situations.” In 1833, Cooper had performed an autopsy on a 10-month-old girl and described right pulmonary hypoplasia, partial right pulmonary arterial supply from the aorta, and partial right lung venous drainage to the inferior vena cava.
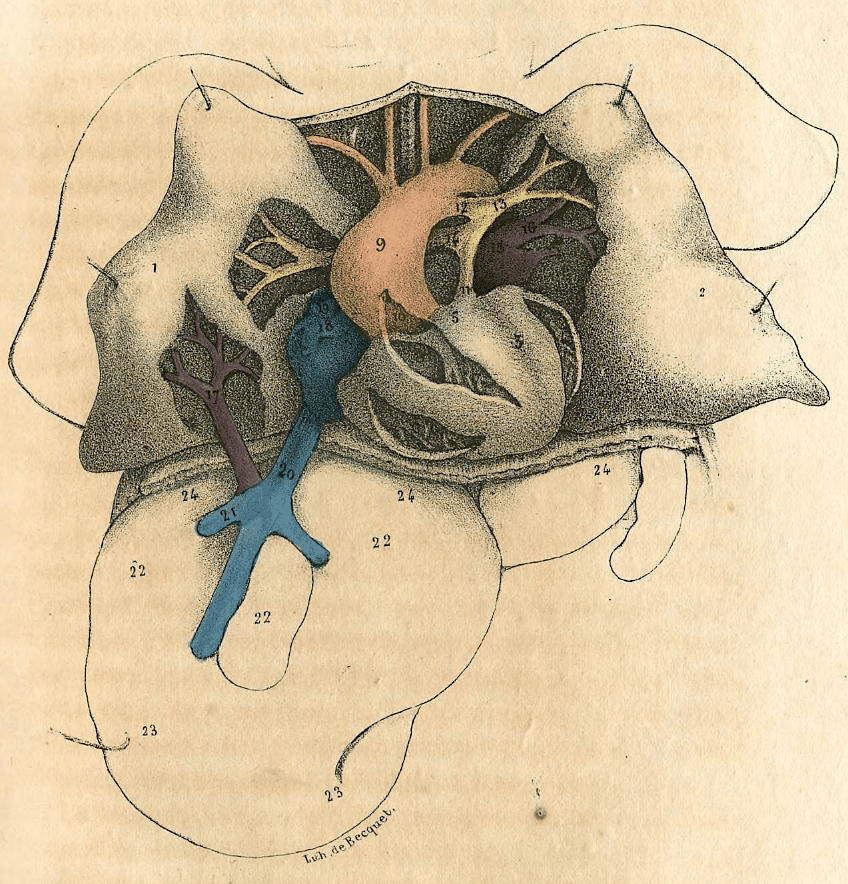
1836 – Raoul Chassinat (1807-1891) accurately defined the anatomy of the anomalous venous return [Legend: in French]
1912 – The pathology of this disease was described in detail by EA Park. He reported the postmortem observation of an anomalous pulmonary venous drainage of the right lung into the diaphragmatic portion of the inferior vena cava in three infant patients
1949 – Dotter et al made the first clinical diagnosis of the anomaly. used the “newly developed technique of venous angiography”, angiocardiography and cardiac catheterization to define the anomalous vessel course In the first published report of the radiographic findings of the “un-named syndrome”, Dotter described the anomaly as
Curving downward through the right lower lung field was a band-like shadow which widened gradually as it descended, paralleling the right cardiac border.
Dotter, 1949: 32
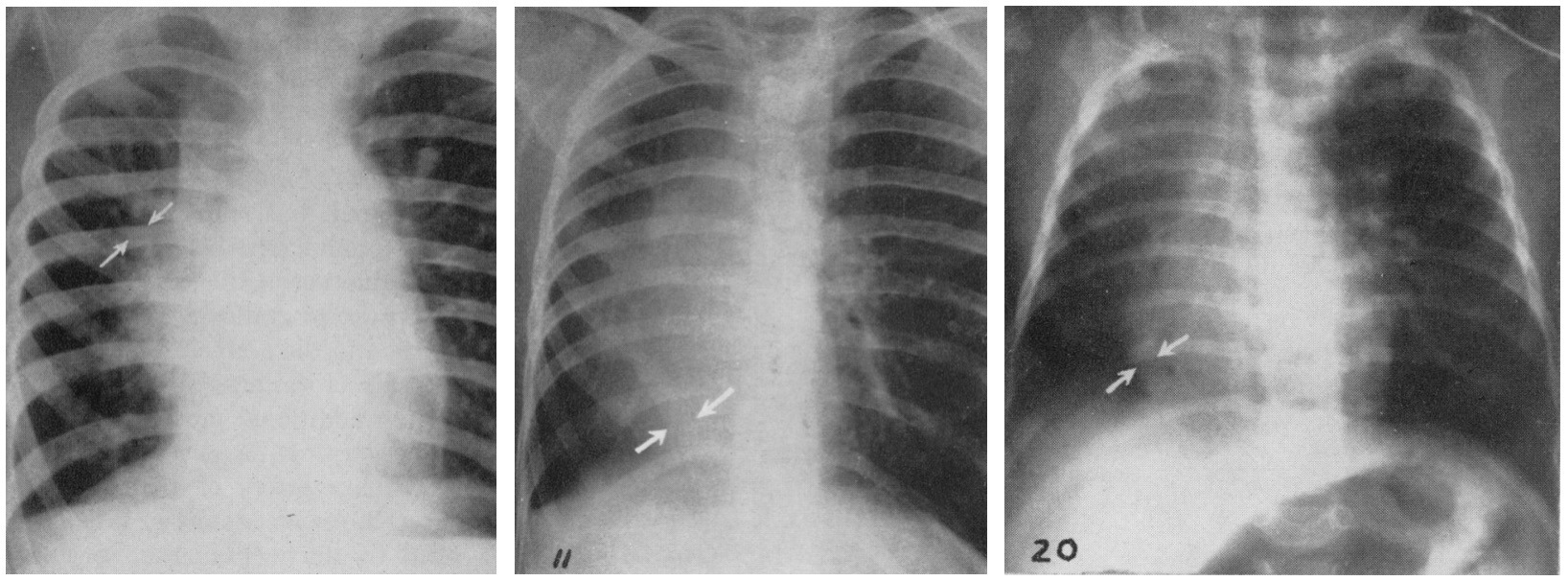
1956 – Halasz et al were the first to actually use the word ‘‘scimitar’’ as a description in their analysis of three cases of anomalous pulmonary venous return to the inferior vena cava. They analysed the clinical, radiographic, circulatory/pulmonary function, and anatomic features in a total of 21 cases.
Radiographic Findings. In the plain films the most striking appearance, which should at once suggest the diagnosis, was that of a dagger or scimitar-shaped vascular density more or less parallel to the right cardiac border, but tending to deviate laterally into the lung field near its tapering upper end (Fig 1, 11, 20)
Halasz. 1956
1960 – Neill et al defined the pathophysiology, clinical findings and familial occurrence and defined two clinically distinct groups of patients. The first groups included sick infants with complications of severe pulmonary hypertension; and the second group compromised typically asymptomatic adults usually incidentally diagnosed following CXR performed for other reasons. Neil termed the condition ‘scimitar syndrome’
Associated Persons
- Catherine Annie Neill (1921 – 2006)
Alternative names
- pulmonary venolobar syndrome
- hypogenetic lung syndrome
References
- Cooper G. Case of malformation of the thoracic viscera consisting of imperfect development of the right lung and transposition of the heart. London Medical Gazette. 1836; 18: 600-602
- Chassinat R. Observation d’anomalies anatomiques remarquables de l’appareil circulatoire, avec hépatocèle congéniale, n’ayant donné lieu pendant la vie à aucun symptôme particulier. Archives générales de médecine 1836; 41: 80-91
- Park EA. Defective development of the right lung due to anomalous development of the right pulmonary artery and vein, accompanied by dislocation of the heart simulating dextrocardia. Proc NY Pathol Soc 1912; 12: 88-93
- Dotter CT, Hardisty NM, Steinberg I. Anomalous right pulmonary vein entering the inferior vena cava; two cases diagnosed during life by angiocardiography and cardiac catheterization. Am J Med Sci. 1949; 218(1): 31-36.
- Halasz NA, Halloran KH, Liebow AA. Bronchial and arterial anomalies with drainage of the right lung into the inferior vena cava. Circulation. 1956;14:826-846.
- Neill CA. Development of the pulmonary veins; with reference to the embryology of anomalies of pulmonary venous return. Pediatrics. 1956;18(6):880-887.
- Neill CA, Ferencz C, Sabiston DC, Sheldon H. The familial occurrence of hypoplastic right lung with systemic arterial supply and venous drainage “scimitar syndrome”. Bull Johns Hopkins Hosp. 1960;107:1-21
- Sanger PW, Taylor FH, Robicsek F. The “Scimitar Syndrome”Diagnosis and Treatment. Arch Surg. 1963; 86(4):580-587
- Mulligan ME. History of scimitar syndrome. Radiology. 1999;210(1):288-290.
- Holt PD, Berdon WE, Marans Z, Griffiths S, Hsu D. Scimitar vein draining to the left atrium and a historical review of the scimitar syndrome. Pediatr Radiol. 2004;34(5):409-413
- Midyat L, Demir E, Aşkin M, et al. Eponym. Scimitar syndrome. Eur J Pediatr. 2010;169(10):1171-1177
- Thiene G. Historical Notes. In: The Complete Reference for Scimitar Syndrome. 2017: 9-15

eponymictionary
the names behind the name
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |
