
![]()
Seizures, Somnolence and a Scary ECG
aka ECG Exigency 006
An 18-year old male is brought to ED by ambulance following a generalised seizure at home. He has a further witnessed seizure en route in the ambulance.
By the time of arrival to ED he is comatose with a GCS of 3 and poor respiratory effort. Pupils are symmetrically dilated. Blood sugar is normal. BP is 70/40.
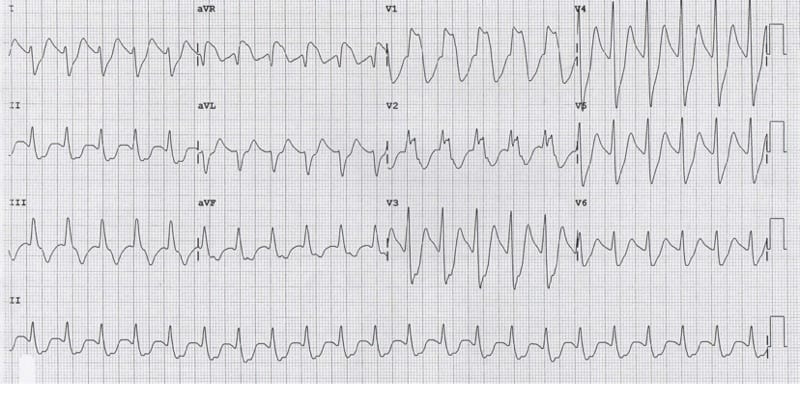
His ECG is shown below:
Questions
Q1. Describe the ECG findings.
The ECG shows:
- Regular broad complex tachycardia
- Rate 130 bpm
- Right axis deviation (+120 degrees)
- Hidden P waves buried in the ST-segments / T waves (best seen in leads II, aVF). These could be retrograde P waves from a junctional / ventricular rhythm or sinus P waves with an extremely long PR interval (360ms)
- Very broad QRS complexes (160ms)
- Terminal R wave in aVR > 3mm; R/S ratio in aVR > 0.7
- Atypical RBBB pattern in V1-2 (bizarre morphology with left rabbit ear higher than the right)
- QT 400ms with markedly prolonged QTc 590 ms
- Non-specific T wave abnormalities with T-wave inversions in V1-2 & lead III
Q2. What is the likely diagnosis?
he combination of tachycardia, QRS and QTc prolongation, right axis deviation and terminal R wave in aVR > 3mm is highly specific for poisoning with sodium-channel blocking drugs, in particular the tricyclic antidepressants.
This patient had attempted suicide by deliberate self-poisoning with around 35mg/kg of Doxepin (a tricyclic antidepressant) an hour prior to presentation.In overdose, the tricyclics produce rapid onset (within 1-2 hours) of:
- Sedation and coma
- Seizures
- Hypotension
- Tachycardia
- Broad complex dysrhythmias
- Anticholinergic syndrome
Tricyclics mediate their cardiotoxic effects via blockade of myocardial fast sodium channels (QRS prolongation, tall R wave in aVR), inhibition of potassium channels (QTc prolongation) and direct myocardial depression. Other toxic effects are produced by blockade at muscarinic (M1), histamine (H1) and α1-adenergic receptors.
The degree of QRS broadening on the ECG is correlated with adverse events:
- QRS > 100 ms is predictive of seizures
- QRS > 160 ms is predictive of ventricular arrhythmias (e.g. VT)
The risk assessment for Doxepin ingestion is as follows:
- < 5 mg/kg — Minimal symptoms
- 5-10 mg / kg — Drowsiness and mild anticholinergic effects; major toxicity not expected
- > 10 mg / kg — Potential for all major toxic effects to occur within 1-2 h of ingestion
- > 30 mg / kg — Severe toxicity with pH-dependent cardiotoxicity and coma > 24 h
An overdose of this magnitude (> 30 mg/kg) is associated with profound TCA toxicity and likely to be rapidly fatal without intervention.
Q3. How would you manage this patient?
Management:
- This patient needs to be managed in a monitored area equipped for airway management and resuscitation.
- Secure IV access, administer high flow oxygen and attach monitoring equipment.
- Administer IV sodium bicarbonate 100 mEq (1-2 mEq / kg); repeat every few minutes until BP improves and QRS complexes begin to narrow.
- Intubate as soon as possible.
- Hyperventilate to maintain a pH of 7.50 – 7.55.
- Once the airway is secure, place a nasogastric tube and give 50g (1g/kg) of activated charcoal.
- Treat further seizures with IV benzodiazepines (e.g. diazepam 5-10mg).
- Treat hypotension with a crystalloid bolus (10-20 mL/kg). If this is unsuccessful in restoring BP then consider starting vasopressors (e.g. noradrenaline infusion).
- If arrhythmias occur, the first step is to give more sodium bicarbonate. Lidocaine (1.5mg/kg) IV is a second line agent once pH is > 7.5.
- Avoid Ia (procainamide) and Ic (flecainide) antiarrhythmics, beta-blockers and amiodarone as they may worsen hypotension and conduction abnormalities.
- Admit the patient to the intensive care unit for ongoing management.
References
LITFL: Toxicology Conundrum 022 – Tricyclic antidepressant (TCA) toxicity.

CLINICAL CASES
ECG Exigency
Emergency Physician in Prehospital and Retrieval Medicine in Sydney, Australia. He has a passion for ECG interpretation and medical education | ECG Library |