
![]()
Serratus Anterior Plane Block
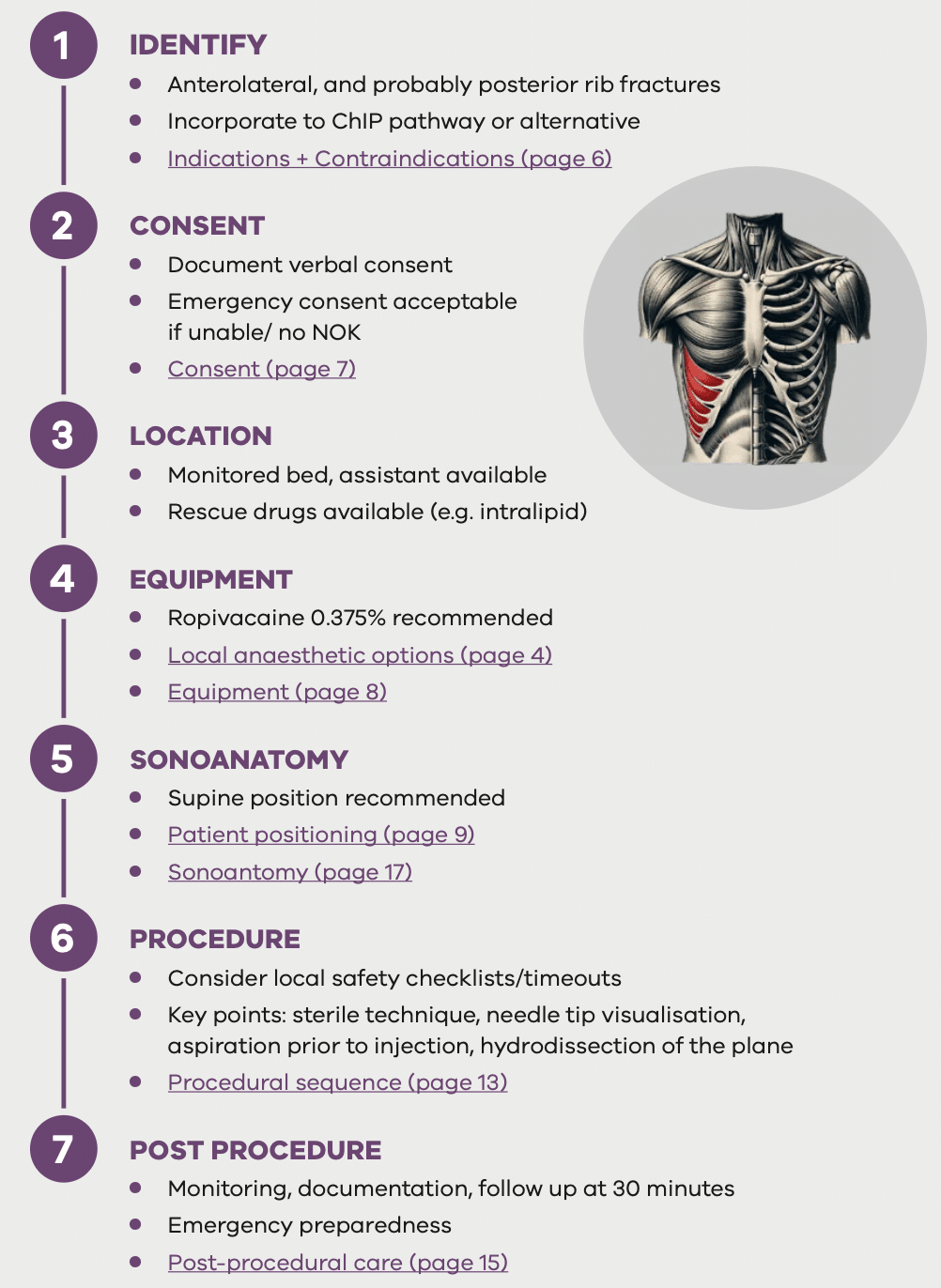
The serratus anterior plane block (SAPB) is an ultrasound-guided regional anaesthesia technique that can transform rib fracture care. By targeting the lateral cutaneous branches of the intercostal nerves, it provides analgesia to most of the ipsilateral hemithorax and can rapidly shift patients from “can’t breathe” to “can cough”, with a much higher proportion achieving pain scores below the “moderate” range.
Together with Dr Daniel Gaetani, Dr Timothy Manion and Prof Kate Curtis, we’ve put together a FOAMed, evidence-based education package on SAPB for emergency clinicians. It’s designed so local experts can focus on teaching and implementation, without having to reinvent the wheel.
The package walks you through a simple seven-step pathway – Identify, Consent, Location, Equipment, Sonoanatomy, Procedure and Post-procedure care – and covers everything from indications, contraindications and local anaesthetic dosing, to ultrasound anatomy, video walkthroughs, and a practical training and credentialling framework.
This guide assumes you’re already comfortable with the basics of plane blocks (aseptic technique, risk management, monitoring after high-dose local anaesthetic, ultrasound use) and shows you how to apply those skills specifically to the serratus anterior plane block in the ED.
References
FOAMed
- Miers J, Partyka C. Procedure: Serratus Anterior Block. LITFL
- Partyka C, Gaetani D, Manion T, Curtis K. Serratus Anterior Plane Block. LITFL
Journals
- Partyka C, Asha S, Berry M, Ferguson I, Burns B, Tsacalos K, Gaetani D, Oliver M, Luscombe G, Delaney A, Curtis K. Serratus Anterior Plane Blocks for Early Rib Fracture Pain Management: The SABRE Randomized Clinical Trial. JAMA Surg. 2024 Jul 1;159(7):810-817.
- Partyka C, Asha S, Berry M, Ferguson I, Burns B, Tsacalos K, Gaetani D, Oliver M, Luscombe G, Delaney A, Curtis K. Serratus Anterior Plane Blocks for Early Rib Fracture Pain Management: The SABRE Randomized Clinical Trial. JAMA Surg. 2024 Jul 1;159(7):810-817.
- Partyka C, Miller M, Burgess S, Drury K, Delaney A, Curtis K. Anatomical Location of Rib Fractures and Associated Analgesic Benefits Achieved From Serratus Anterior Plane Blocks: A Spatial Point Pattern Analysis. Anesth Analg. 2025 Jan 1;140(1):231-234
- Curtis K, Asha SE, Unsworth A, Lam M, Goldsmith H, Langcake M, Dwyer D. ChIP: An early activation protocol for isolated blunt chest injury improves outcomes, a retrospective cohort study. Australas Emerg Nurs J. 2016 Aug;19(3):127-32
- Harrington C, Bliss J, Lam L, Partyka C. Serratus Anterior Plane Block for Clinically Suspected Rib Fractures in Prehospital and Retrieval Medicine. Prehosp Emerg Care. 2024;28(1):30-35
Emergency Procedures

Dr Chris Partyka MBBS, BMedSci, MD. Staff Specialist in Emergency Medicine, Royal North Shore Hospital. Prehospital and Retrieval Specialist, NSW Ambulance. Clinical Lecturer, University of Sydney
Hi Chris
I am a big fan of regional nerve blockade however I don’t use SAP blocks (or ESPs) because I am unconvinced of their utility for rib fractures.
The main problem with the SABRE trial is that it isn’t blinded. Therefore it’s open to placebo effect and operator bias (because the delivering clinicians recorded the pain scores, and they are likely to be US enthusiasts, so of course they want the blocks to work).
Inevitably the anaesthetic will numb the overlying tissue and the patient may perceive this as a reduction in pain. But a superficial SAP block is deposited on the other side of a muscle plane from the broken ribs, and I find it biomechanically implausible that this will reach the intercostal nerves – because there are another 3 layers of intercostal muscle to get through.
A placebo effect would also explain why the blocks seemed to work on posterior fractures, why the analgesic effect lasted longer than ropivacaine would be expected to, and why they only helped 20% of patients – and only then to a moderate degree.
If SAP blocks actually worked on the intercostal nerves, you wouldn’t just get a 2/10 reduction in pain score: the patient would be pain-free because there are no other nerves involved. Perhaps there is some spread through disrupted tissue planes to the fracture sites. So SAPs might work like haematoma blocks. Or perhaps reduce pain from overlying contused soft tissue.
I’ve used US guided intercostal blocks for rib fractures to much better effect (typically complete analgesia). But they are tricky, time-consuming, wear off fast, require high doses of LA if multiple ribs are involved so there is a risk of LAST, and you have to get really close to the pleura. Therefore I’m not convinced that intercostal blocks are useful in the ED, either.
I appreciate that this is a difficult subject to research, and that great effort has gone in. However I don’t think SABRE can justify bringing in SAP blocks as part of standard treatment for rib fractures. I think SAPs are fine for chest wall surgery, which was their original purpose, and for which there is good rationale and stronger evidence.
Cheers
Jo