
![]()
Shock, syncope and severe chest pain
aka ECG Exigency 014
A 67-year old male is brought to hospital by ambulance following an episode of syncope at home. He had just finished eating lunch at home when he developed severe crushing retrosternal chest pain radiating to his left arm, profuse sweating and vomiting.
Shortly after the onset of the pain he lost consciousness and awoke to find himself on the floor. En route in the ambulance he has several brief runs of non-sustained VT associated with dizziness and an impalpable radial pulse.
On arrival to ED, his observations are: BP 80/50, HR 130 regular, SaO2 91% on 15L, RR 30. He looks unwell, grey, sweaty and dyspnoeic. Chest exam reveals bilateral basal crepitations extending to the midzones. Heart sounds are normal with no murmurs. This is his ECG…

Q1. Describe the ECG
Answer and Interpretation
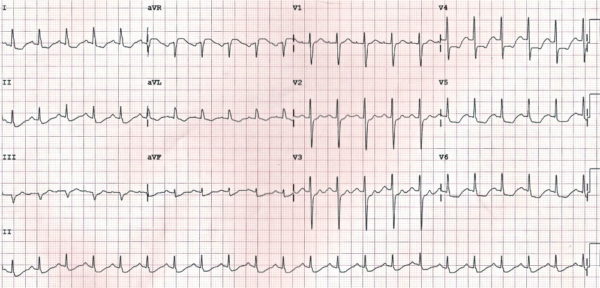
- Sinus tachycardia with two premature supraventricular complexes (“PSVC”) – these are probably atrial in origin as they are both preceded by abnormal P waves (hidden within the preceding T-waves)
- Overall ventricular rate = 108 bpm
- Left axis deviation
- PR interval normal (~160ms)
- Broad QRS (~120ms) secondary to non-specific interventricular conduction delay (not characteristic of LBBB or RBBB); the QRS appears wider than it actually is in some leads due to the upsloping ST segments
- Widespread ST depression in I, II, aVF and V2-6 with T-wave inversion in aVL
- Marked ST elevation in aVR (> 3mm at the J-point)
- In comparison, there is minimal ST elevation in V1 (i.e. STE in aVR > V1)
Q2. What is the significance of the ECG changes?
Answer and Interpretation
In a patient presenting with ischaemic chest pain, the combination of:
- Widespread ST depression
- ST elevation in aVR ≥ 1mm
- ST elevation in aVR ≥ V1
Is strongly suggestive of left main coronary artery (LMCA) occlusion or severe multi-vessel disease.
ST elevation in aVR: Left Main Coronary Artery Occlusion?
This ECG demonstrates the classical pattern of LMCA occlusion:
- Widespread horizontal ST depression, most prominent in leads I, II and V4-6
- ST elevation in aVR ≥ 1mm
- ST elevation in aVR ≥ V1
However, ST elevation in aVR is not entirely specific to LMCA occlusion. It may also be seen with:
- Proximal left anterior descending artery (LAD) occlusion
- Severe triple-vessel disease (3VD)
Q3. What is the electrophysiological basis for the ECG changes?
Answer and Interpretation
Mechanism of STE in aVR
- Lead aVR is electrically opposite to the left-sided leads I, II, aVL and V4-6; therefore ST depression in these leads will produce reciprocal ST elevation in aVR.
- Lead aVR also directly records electrical activity from the right upper portion of the heart, including the right ventricular outflow tract and the basal portion of the interventricular septum; infarction in this area could theoretically produce ST elevation in aVR.
ST elevation is aVR is thought to result from two possible mechanisms:
- Diffuse subendocardial ischaemia (producing reciprocal change in aVR)
- Transmural ischaemia / infarction of the basal interventricular septum (e.g. due to a proximal occlusion within the left coronary system)
NOTE: The basal septum is supplied by the first septal perforator artery (a very proximal branch of the LAD), so ischaemia/infarction of the basal septum would imply involvement of the proximal LAD or LMCA.
Q4. What is the predictive value of these ECG changes?
Answer and interpretation
Predictive Value of STE in aVR
In the context of widespread ST depression + symptoms of myocardial ischaemia:
- STE in aVR ≥ 1mm indicates proximal LAD / LMCA occlusion or severe 3VD
- STE in aVR ≥ 1mm predicts the need for CABG
- STE in aVR ≥ V1 differentiates LMCA from proximal LAD occlusion
- Absence of ST elevation in aVR almost entirely excludes a significant LMCA lesion
In the context of anterior STEMI:
- STE in aVR ≥ 1mm is highly specific for LAD occlusion proximal to the first septal branch
In patients undergoing exercise stress testing:
- STE of ≥ 1mm in aVR during exercise stress testing predicts LMCA or ostial LAD stenosis
Magnitude of ST elevation in aVR is correlated with mortality in patients with acute coronary syndromes:
- STE in aVR ≥ 0.5mm was associated with a 4-fold increase in mortality
- STE in aVR ≥ 1mm was associated with a 6- to 7-fold increase in mortality
- STE in aVR ≥ 1.5mm has been associated with mortalities ranging from 20-75%
In-depth review of relevant literature
A Brief Review of the Literature
Over the past 18 years, multiple studies have examined the utility of ST elevation in aVR for predicting severe coronary artery disease (proximal LAD/LMCA/3VD) and mortality in patients with acute coronary syndromes and those undergoing exercise stress testing. Some of the important studies are summarised below…
- Population: 113 patients with unstable angina, including 20 patients with LMCA stenosis and 24 patients with 3VD.
- Findings: Patients with LMCA or 3VD frequently demonstrated ST-segment depression in multiple leads (typically I, II and V4-V6) plus ST-segment elevation in lead aVR during attacks of angina.
- Population: 100 patients with anterior STEMI.
- Findings: STE in aVR of any magnitude was 43% sensitive and 95% specific for LAD occlusion proximal to the first septal branch.
- Population: 16 patients with acute LMCA occlusion, 46 patients with acute LAD occlusion and 24 patients with acute RCA occlusion.
- Findings:
- STE in aVR (≥ 0.5mm) occurred with a significantly higher incidence in the LMCA group (88%) than in the LAD (43%) or RCA (8%) groups.
- Magnitude of STE in aVR was significantly greater in the LMCA group (1.6 ± 1.3 mm) than the LAD group (0.4 ± 1.0 mm).
- In contrast, magnitude of STE in V1 was less in the LMCA group (0.0 ± 2.1 mm) than in the LAD group (1.4 ± 1.1 mm).
- STE in aVR ≥ V1 distinguished the LMCA group from the LAD group with 81% sensitivity, 80% specificity and 81% accuracy.
- Population: 775 patients with first presentation of acute NSTEMI
- Findings:
- Two-thirds of patients with STE in aVR ≥ 1 mm had either LMCA occlusion or severe 3VD.
- Degree of STE in aVR was an independent predictor of mortality: STE of ≥ 1 mm was associated with a six- to seven-fold increase in in-hospital mortality (odds ratio of death = 6.6).
- Magnitude of STE in aVR was also closely associated with rates of recurrent ischemic events and heart failure.
- STE in aVR predicted the need for CABG – coronary grafting was required in 22% of patients with aVR STE > 1mm compared to 5% of those without.
- Population: 150 patients with acute coronary syndromes – 46 with LMCA obstruction, 104 with occlusion of a different vessel
- Findings: STE in aVR was twice as common in patients with LMCA occlusion as those without (69.6% vs 34.6%).
- Population: 310 patients with non-ST-elevation acute coronary syndromes.
- Findings:
- STE in aVR ≥ 0.5 mm was the strongest predictor of LMCA or 3VD (78% sensitivity, 86% specificity, 57% PPV and 95% NPV).
- STE in aVR was superior to the presence of ST depression in other leads for predicting LMCA/3VD.
- Population: 950 patients with STEMI (any type).
- Findings:
- STE in aVR ≥ 0.5 mm predicted proximal LAD or LMCA occlusion (with 50% sensitivity, 91% specificity, 55% PPV, 89% NPV).
- STE in aVR ≥ 0.5 mm was also an independent predictor of mortality (in-hospital mortality was 19% in those with ≥ 0.5 mm STE in aVR compared to only 5% in those without).
- Patients with STE in aVR also had higher heart rates, lower systolic BPs, lower ejection fractions and worse Killip class at the time of admission.
- Population: 15, 315 patients with STEMI enrolled in the HERO-2 trial (heparin vs bivalirudin for acute MI).
- Findings: STE ≥1.5 mm in aVR was associated with a two-fold increase in 30-day mortality for both inferior and anterior STEMI, compared to the baseline mortality rate of 10.8%.
- Population: 454 patients undergoing both exercise stress testing (standard Bruce protocol) and cardiac catheterization within 6 months, including 75 patients with LMCA or ostial LAD stenosis.
- Findings: STE of ≥ 1mm in aVR during stress testing predicted LMCA or ostial LAD stenosis with sensitivity 75%, specificity 81% and overall accuracy 80%.
- Population: 572 patients with acute NSTEMI.
- Findings:
- Degree of STE in aVR was the strongest independent predictor of severe LMCA occlusion / 3VD requiring CABG (odds ratio 29.1), followed by positive troponin T level (odds ratio 1.27).
- STE ≥ 1.0 mm in aVR identified severe LMCA occlusion /3VD with 80% sensitivity, 93% specificity, 56% PPV, and 98% NPV.
Further ECG examples
More ECG Examples
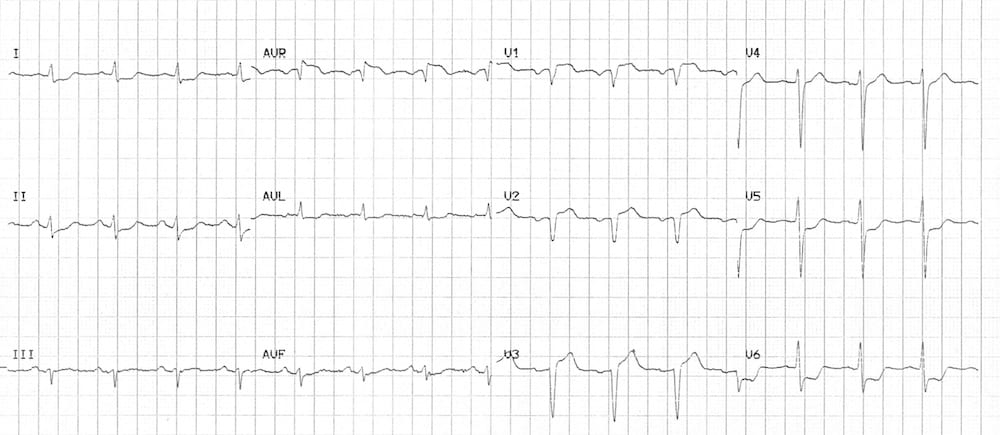
Proximal LAD occlusion

This ECG shows:
- ST elevation in aVR and V1 of similar magnitude.
- Widespread ST depression (V3-6, I, II, III, aVF)
This patient had a severe ostial LAD thrombus that was close to the left main (This ECG is reproduced from Dr Smith’s ECG Blog)
Severe Multi-Vessel Disease
This ECG shows:
- ST elevation in aVR and V1, of similar magnitude
- ST depression in multiple leads (V5-6, I, II, aVL, aVF)
- Evidence of anteroseptal STEMI – ST elevation with Q wave formation in V1-3
It would be reasonable to suspect a proximal LAD occlusion based on this ECG. However, this patient actually had severe multi-vessel disease. Angiography demonstrated a chronic total occlusion of his circumflex artery, with critical stenoses of his proximal LAD, RCA and ramus intermedius. Surprisingly, in this case the culprit vessel was thought to be the RCA, which had been collateralising his chronically occluded circumflex.
Q5. What are the implications of this ECG pattern for the treatment of acute coronary syndromes?
Answer and interpretation
Implications for therapy in acute coronary syndromes
Given the ability of STE in aVR to predict critical coronary lesions and death, this ECG pattern is increasingly being recognised as a “STEMI equivalent” that requires emergent reperfusion therapy to prevent cardiogenic shock and death. Furthermore, the presence or absence of STE in aVR may potentially inform the decision to give thienopyridine platelet inhibitors (e.g. clopidogrel, prasugrel) during an acute coronary syndrome:
- Clopidogrel treatment ≤ 7 days before CABG is associated with an increase in major bleeding, haemorrhage-related complications, and transfusion requirements.
- Prasugrel is associated with even more bleeding than clopidogrel.
- If urgent CABG (within 7 days) is likely, then there is an argument for omitting thienopyridines during the initial management of an acute coronary syndrome (or at least using clopidogrel instead of prasugrel).
In the study by Kosuge et al. (2011)
- STE in aVR ≥ 1 mm was a strong predictor of severe LMCA / 3VD requiring CABG.
- Conversely, patients with < 1mm ST elevation in aVR had a negligible risk of severe LMCA / 3VD requiring CABG.
Based on this data:
- Patients with < 1mm STE in aVR may safely receive clopidogrel/prasugrel during the initial treatment of their ACS as they are unlikely to proceed to urgent CABG.
- Patients with ≥ 1 mm STE in aVR may potentially require early CABG; therefore these patients should ideally be discussed with the interventional cardiologist (± cardiac surgeon) before thienopyridines are given.
Q6. Can you guess what happened next?
Reveal answer
- There was some initial resistance to urgent angiography as the junior cardiology registrar failed to appreciate the significance of the ECG changes.
- Luckily for the patient, the astute Emergency Physician persisted…
- Shortly after showing the ECG to his boss, a rather panicky cardiology registrar ran into ED and whisked the patient off to the cath lab!
- Coronary angiogram showed a complete ostial occlusion of the LMCA, with acute thrombus. The remainder of the coronary arteries were normal, apart from some minor irregularities in the RCA.
- The patient stabilised after PCI to the LMCA.
- An intra-aortic balloon pump (IABP) was inserted at the time of angiography and remained in situ for two days while the patient recovered from his cardiogenic shock.
- Troponin peaked at 220 μg/L.
- The patient made a good recovery – echocardiography performed six days later showed normal LV size with only mild segmental systolic dysfunction and an ejection fraction of 48%.
- He was transferred to a private hospital for ongoing management, so I am not sure whether he ultimately required CABG.
References
…there are a lot
- Aygul N, Ozdemir K, Tokac M, Aygul MU, Duzenli MA, Abaci A et al. Value of lead aVR in predicting acute occlusion of proximal left anterior descending coronary artery and in-hospital outcome in ST-elevation myocardial infarction: an electrocardiographic predictor of poor prognosis. J Electrocardiol. 2008 Jul-Aug;41(4):335-41 [abstract].
- Barrabes JA, Figueras J, Moure C, Cortadellas J, Soler-Soler J. Prognostic value of lead aVR in patients with a first non-ST-segment ele- vation acute myocardial infarction. Circulation 2003; 108: 814 – 819 [full text].
- Chan TC, Brady WJ, Harrigan RA, Ornato JP and Rosen PR. ECG in Emergency Medicine and Acute Care. Elsevier 2005.
- Engelen DJ, Gorgels AP, Cheriex EC, De Muinck ED, Ophuis AJ, Dassen WR et al. Value of the electrocardiogram in localizing the occlusion site in the left anterior descending coronary artery in acute anterior myocardial infarction. J Am Coll Cardiol. 1999 Aug;34(2):389-95 [full text].
- Eskola MJ, Nikus KC, Holmvang L, et al. Value of the 12-lead electrocardiogram to define the level of obstruction in acute anterior wall myocardial infarction: Correlation to coronary angiography and clinical outcome in the DANAMI-2 trial. Int J Cardiol 2009;131:378–383 [abstract].
- Gorgels AP, Engelen DJ, Wellens HJ. Lead aVR, a mostly ignored but very valuable lead in clinical electrocardiography. J Am Coll Cardiol. 2001 Nov 1;38(5):1355-6 [full text].
- Gorgels AP, Vos MA, Mulleneers R, de Zwaan C, Bär FW, Wellens HJ. Value of the electrocardiogram in diagnosing the number of severely narrowed coronary arteries in rest angina pectoris. Am J Cardiol. 1993 Nov 1;72(14):999-1003 [abstract].
- Gul EE, Nikus KC. An unusual presentation of left anterior descending artery occlusion: significance of lead aVR and T-wave direction. J Electrocardiol. 2011 Jan-Feb;44(1):27-30 [full text].
- Hennings JR, Fesmire FM. A new electrocardiographic criteria for emergent reperfusion therapy. Am J Emerg Med. 2011 Jun 22. Epub ahead of print [abstract].
- Jong G, Ma T, Chou P, et al. Reciprocal changes in 12-lead electrocardiography can predict left main coronary artery lesion in patients with acute myocardial infarction. In Heart J 2006;47:13-20
- Kireyev D, Arkhipov MV, Zador ST, Paris JA, Boden WE. Clinical utility of aVR-The neglected electrocardiographic lead. Ann Noninvasive Electrocardiol. 2010 Apr;15(2):175-80 [abstract]
- Kosuge M, Ebina T, Hibi K, Endo M, Komura N, Hashiba K et al. ST-segment elevation resolution in lead aVR: a strong predictor of adverse outcomes in patients with non-ST-segment elevation acute coronary syndrome. Circ J. 2008 Jul;72(7):1047-53
- Kosuge M, Ebina T, Hibi K, Morita S, Endo M, Maejima N, et al. An early and simple predictor of severe left main and/or three-vessel disease in patients with non-ST-segment elevation acute coronary syndrome. Am J Cardiol. 2011 Feb 15;107(4):495-500 [abstract].
- Kosuge M, Kimura K, Ishikawa T, Ebina T, Shimizu T, Hibi K, et al. Predictors of left main or three-vessel disease in patients who have acute coronary syndromes with non-ST-segment elevation. Am J Cardiol 2005; 95: 1366 – 1369 [abstract].
- Kosuge M, Kimura K, Ishikawa T, Ebina T, Hibi K, Tsukahara K, et al. Combined prognostic utility of ST segment in lead aVR and troponin T on admission in non-ST-segment elevation acute coronary syndromes. Am J Cardiol 2006; 97: 334 – 339 [abstract].
- Kosuge M, Ebina T, Hibi K, Morita S, Komura N, Hashiba K et al. Early, accurate, non-invasive predictors of left main or 3-vessel disease in patients with non-ST-segment elevation acute coronary syndrome. Circ J. 2009 Jun;73(6):1105-10 [full text].
- Kühl JT, Berg RM. Utility of lead aVR for identifying the culprit lesion in acute myocardial infarction. Ann Noninvasive Electrocardiol. 2009 Jul;14(3):219-25 [abstract].
- Nikus KC, Eskola MJ. Electrocardiogram patterns in acute left main coronary artery occlusion. J Electrocardiol. 2008 Nov-Dec;41(6):626-9 [abstract].
- Ozmen N, Yiginer O, Uz O, Kardesoglu E, Aparci M, Isilak Z et al. ST elevation in the lead aVR during exercise treadmill testing may indicate left main coronary artery disease. Kardiol Pol. 2010 Oct;68(10):1107-11 [abstract].
- Pickard AS, Becker RC, Schumock GT, Frye CB. Clopidogrel-associated bleeding and related complications in patients undergoing coronary artery bypass grafting. Pharmacotherapy. 2008 Mar;28(3):376-92 [abstract].
- Rostoff P, Piwowarska W, Konduracka E, Libionka A, Bobrowska- Juszczuk M, Stopyra K, et al. Value of lead aVR in the detection of significant left main coronary artery stenosis in acute coronary syndrome. Kardiol Pol 2005;62:128-37 [abstract].
- Uthamalingam S, Zheng H, Leavitt M, Pomerantsev E, Ahmado I, Gurm GS, Gewirtz H. Exercise-induced ST-segment elevation in ECG lead aVR is a useful indicator of significant left main or ostial LAD coronary artery stenosis. JACC Cardiovasc Imaging. 2011 Feb;4(2):176-86 [abstract].
- de Winter RJ, Verouden NJW, Wellens HJJ, Wilde AAM. A new sign of proximal LAD occlusion. N Engl J Med 2008;359:2071-3 [full text].
- Wiviott SD, Braunwald E, McCabe CH, Montalescot G, Ruzyllo W, Gottlieb S, et al. TRITON-TIMI 38 Investigators. Prasugrel versus clopidogrel in patients with acute coronary syndromes. N Engl J Med. 2007 Nov 15;357(20):2001-15 [abstract].
- Williamson K, Mattu A, Plautz CU, Binder A, Brady WJ. Electrocardiographic applications of lead aVR. Am J Emerg Med. 2006 Nov;24(7):864-74 [pdf].
- Wong CK, Gao W, Stewart RA, French JK, Aylward PE, White HD; for the HERO-2 Investigators. The prognostic meaning of the full spectrum of aVR ST-segment changes in acute myocardial infarction. Eur Heart J. 2011 Aug 19 [abstract].
- Yamaji H, Iwasaki K, Kusachi S, Murakami T, Hirami R, Hamamoto H, et al. Prediction of acute left main coronary artery obstruction by 12-lead electrocardiography. ST segment elevation in lead aVR with less ST segment elevation in lead V(1). J Am Coll Cardiol. 2001 Nov 1;38(5):1348-54 [full text].
Further Reading
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF

CLINICAL CASES
ECG EXIGENCY
Emergency Physician in Prehospital and Retrieval Medicine in Sydney, Australia. He has a passion for ECG interpretation and medical education | ECG Library |

Ed
another extraordinary case!
and excellent presentation. this was a great save, thanks to the persistence of the ED doc.
perhaps i was mistaken in my comment elsewhere (i think it was the widow-maker blog).
this case clearly shows a man who had “complete” OMI, involving the os to the LM.
and an ECG that had marked ST elevation aVR.
question, ED…
tell me if i’m mistaken.
i think the actual QRS width determination is best seen in leads aVL and V1, which makes the QRS nearly normal width, but it we “march” this width out to the other leads it dramatically illustrates the severe ST elevation in aVR, and depression elsewhere.
get post, ED. thank you.
tom
What would you do in a “rural” setting with no access to PCI for >2-3hr. Would you give lytics or hold off?