
![]()
Théodore Tuffier

Théodore-Marin Tuffier (1857-1929) was a French surgeon
Tuffier was a surgeon of the Paris school whose career bridged the late-19th-century era of “heroic” operative surgery and the early 20th-century turn toward physiology-driven technique. Trained in a tradition that valued audacity at the operating table, he paired technical confidence with an unusually experimental outlook, repeatedly testing surgical ideas against the practical limits of ventilation, circulation and shock.
As a surgeon, Tuffier was best known for ambitious work in intrathoracic and cardiovascular surgery at a time when entering the chest was still regarded as perilous. He published and taught on pulmonary surgery and operative access, pursued physiological solutions to the problem of operating with pneumothorax. He reported early open-chest cardiac compression (“massage du cœur”) as a rescue manoeuvre after profound collapse and experimental heart-valve surgery, with Alexis Carrel. Later historical accounts also associate his name with thoracic instrumentation and exposure techniques that matured during the wartime period, reflecting his focus on making the chest surgically “approachable.”
Tuffier’s influence on anaesthesia and procedural medicine came from the same instinct: standardise the method, then build the tools. He became an early proponent of spinal anaesthesia (rachicocaïnisation) publishing on technique, indications, complications and sterility, and specifying a purpose-built long lumbar needle. His name persists in everyday clinical anatomy through Tuffier’s (intercristal) line, and in device history through practical innovations such as a chloroform inhaler and lumbar spinal needle.
Biographical Timeline
- Born March 26, 1857 in Bellême, Orne, France.
- 1879 – Interne des hôpitaux (Paris hospitals).
- 1880 – Vice-president, Société anatomique.
- 1881 – Prosecteur (Faculty of Medicine).
- 1885 – MD (Docteur en médecine); laureate of the Faculty (thesis – Du rôle de la congestion dans les maladies des voies urinaires).
- 1887 – Appointed chirurgien des hôpitaux. Officier d’Académie; also Prix d’Argenteuil (Académie de Médecine).
- 1889 – Professeur agrégé (Faculty of Medicine, Paris).
- 1892 – Member, Société de chirurgie (later secretary 1904; vice-president 1913).
- 1893 – Chevalier de la Légion d’honneur.
- 1897 – Rapporteur, Moscow surgical congress; awarded Prix Laborie (with Hallion).
- 1898 – At La Pitié, performed a dramatic early clinical attempt at open cardiac massage
- 1900 – Presented/advanced spinal “cocaine analgesia” by rachidian route in Paris
- 1900–1908 – Created and delivered a course in experimental surgery (free course) at the Faculty of Sciences.
- 1900–1913 – Chargé de cours complémentaire de clinique chirurgicale, Hôpital Beaujon.
- 1902–1906 – International society memberships and congress roles (e.g., honorary member Russian Society of Surgery of Pirogoff; associated Belgian society; etc.).
- 1911 – Officier de la Légion d’honneur.
- 1913 – Elected Fellow of the Royal College of Surgeons (London)
- 1914–1918 – Major Great War service: reorganised surgical services; drove adoption of modern wound care and inter-allied coordination; chaired/organised Interallied Surgical Conferences (first held May 1916 in Paris).
- 1920 – British honours for allied war work: Honorary KBE and Companion of the Bath (CB)
- 1925 – Jubilee celebrations at the Third International Congress of Medicine and Pharmacy
- Died October 27, 1929, Paris, France.
Medical Eponyms
Tuffier’s line (Jocoby’s line)
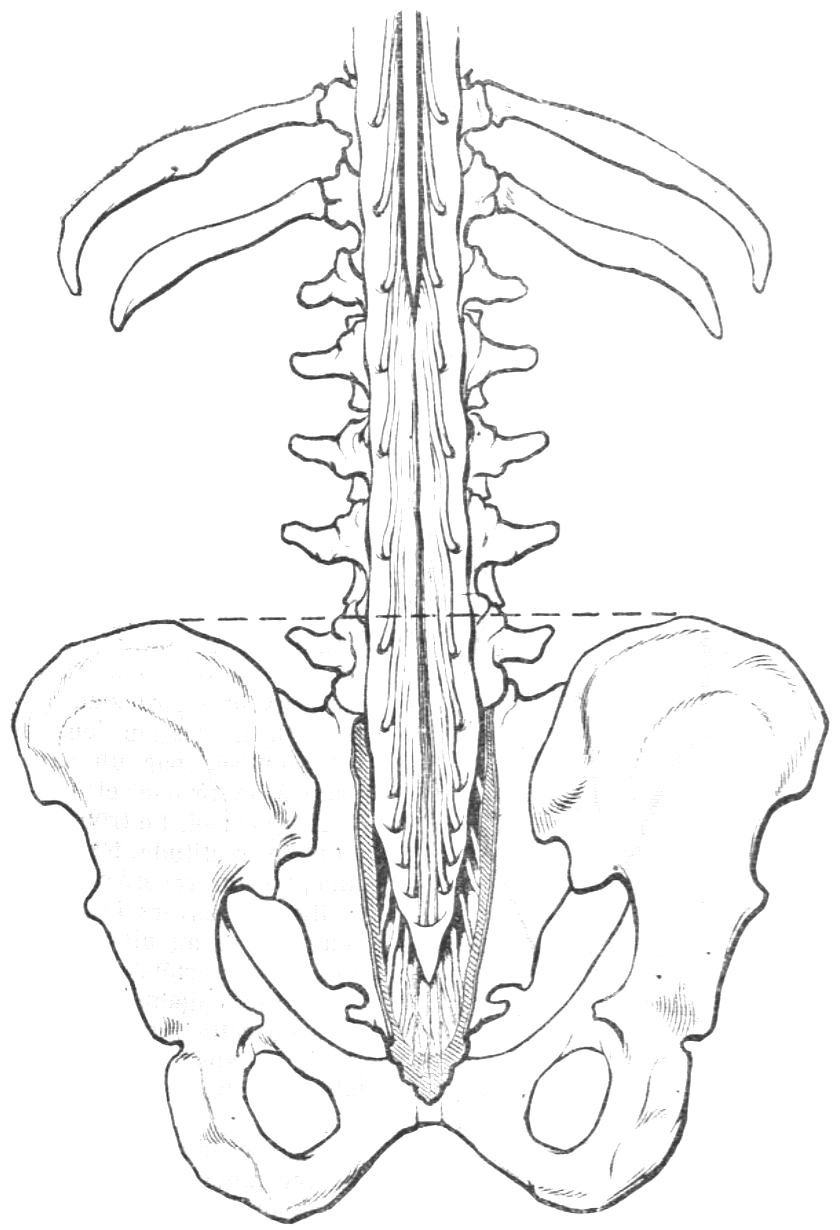
A transverse line joining the highest points of both iliac crests (intercristal/supracristal line), used as a surface landmark to estimate lumbar level for lumbar puncture, spinal anaesthesia, and epidural placement.
1895 – George W Jacoby (1856-1940) described the line as a practical landmark for lumbar puncture, stating that a line drawn between the highest points of the iliac crests passes through the centre of the fourth lumbar vertebra (L4) (often termed Jacoby’s line, particularly in Japan)
…a line drawn across and joining the highest point of both cristae ilii will pass through the centre of the fourth lumbar vertebra…
Jacoby 1895
1900 – Tuffier described the same bony landmark in the context of spinal cocaine injection (“anesthésie médullaire…”) and illustrated its use. In his figure, the dotted line emphasises the anatomical rationale for lumbar puncture/spinal injection: the subarachnoid cul-de-sac extends below the end of the spinal cord, which ends at the inferior border of L1.
Je pratique depuis le 9 novembre 1899 l’anesthésie chirurgicale par injection de cocaïne dans l’espace sous-arachnoïdien lombaire…La ligne pointillée indique… le cul-de-sac arachnoïdien, la moelle se terminant au bord inférieur de la première lombaire
Tuffier, 1900
Modern interpretation: Radiographic and cadaver studies demonstrate that the intercristal line is variable, most commonly corresponding to L4, L4–5, or L5, with clinically meaningful spread (including cases higher than expected).
Clinical takeaway: Treat the line as a rough guide, not a guarantee of L4/5—particularly when trying to avoid an unintentionally high neuraxial level. Ultrasound/imaging improves accuracy where precision matters.
Tuffier inhaler (1905)
A metal chloroform inhaler designed to deliver chloroform more continuously and in a controlled manner, aiming to reduce the dose fluctuations seen with many contemporary inhalers and the open-drop technique.
1905 – Tuffier introduced his inhaler at a meeting of the Société de Chirurgie de Paris, following several months of testing and modification with the instrument maker Collin.
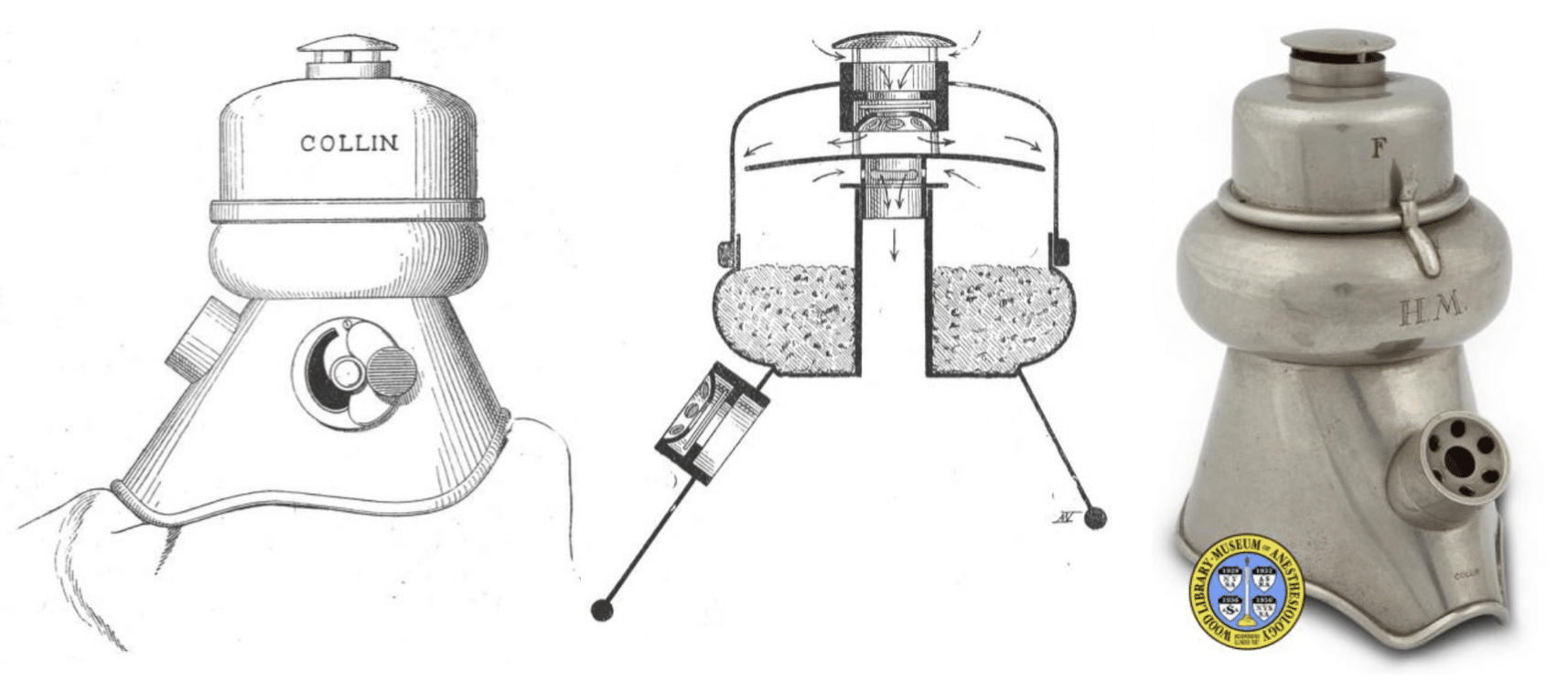
Right: Photograph of inhaler: Wood Library-Museum of Anesthesiology
Tuffier’s rationale was explicitly dose stability: he believed fluctuating chloroform delivery increased adverse effects, and designed an apparatus to smooth and control administration during surgery.
The Tuffier inhaler illustrates the early 20th-century push toward measured, reproducible inhalational anaesthesia delivery, at a time when chloroform safety was a dominant concern.
Key Medical Contributions
Spinal anaesthesia and rachicocaïnisation (1899–1904)
Tuffier was one of the earliest surgeons to operationalise subarachnoid cocaine injection as a reproducible anaesthetic technique for mainstream surgery. In his 1900 reports, Tuffier states “Après de nombreuses recherches, je pratique depuis le 9 novembre 1899 l’anesthésie chirurgicale par injection de cocaïne…(Société de biologie)”. He presented a substantial early series (63 cases in Semaine médicale) across lower limb, perineal/rectal and genitourinary operations arguing the method was practical and could enter routine practice.
Technique and the “Tuffier needle”
A recurring theme in Tuffier’s spinal writing is standardising the anaesthetic kit and the process involved. IHe specifies a sterilizable syringe and a purpose-made needle designed for the realities of lumbar puncture: long enough to reach the subarachnoid space in variable body habitus, stiff enough not to bend when the laminae are contacted, and with a short bevel to reduce partial extra-dural injection through a long oblique orifice. He gives specific measurements (length and internal/external diameters) for the needle.

That device lineage persists in museum collections: a “Tuffier’s lumbar needle in holder,” made in Paris by Collin et Compagnie, dated 1901–1930 (nickel-plated steel).
Scaling up, complications, and a “clean” mixing method
Tuffier refines the technique adjusting solution strength, asepsis, puncture level, and patient positioning and helped expand the operative field (including increasingly major surgery). In 1902, his “technique actuelle” emphasises rigorous asepsis, explicitly rejecting open-air mixing of cocaine solution and CSF as “dangerous.” He describes a practical workflow using standardised ampoules (4 centigrammes cocaine in 7 drops sterile water; ~12%), aspirated into a Luer syringe, followed by puncture; once CSF flows, the syringe is attached and allowed to fill with CSF (piston pushed back), then the fully mixed contents are injected slowly back intrathecally.
Chest surgery, cardiac massage and operative access to the thorax
Tuffier worked on intrathoracic technique at a time when pneumothorax, bleeding control, and ventilation were the limiting factors, and he repeatedly tried to solve these problems at the interface of physiology and surgery.
1896 – His early collaboration with Hallion on Operations intrathoraciques avec respiration artificielle par insufflation sits squarely in this tradition: not simply “doing chest surgery,” but building the physiological conditions that made it possible.
1898 – Tuffier and Hallion described chloroform syncope treated by opening the chest and performing rhythmic manual compression of the heart (“massage du cœur”) until spontaneous systoles returned and respiration reappeared. They presented the manoeuvre not as a laboratory curiosity but as a potential salvage technique for otherwise fatal collapse when standard methods had failed.
1913 – Tuffier worked with Alexis Carrel at the Rockefeller Institute, undertaking experimental operations aimed at relieving valvular stenosis by mechanical means. In the report published the following year he describes external valvulotomy, incising the aortic or pulmonary ring from without, and using an arterial patch sutured on three sides before opening the vessel/valve and then rapidly closing the fourth side, with most animals surviving.
1922 – Tuffier’s legacy in thoracic surgery also includes instrumentation and access. Later accounts link him with self-retaining rib-spreading technology and with a bilateral transsternal extension of thoracotomy later referred to as “Tuffier’s method”, a wartime-influenced lineage that anticipates modern bilateral anterior thoracic exposure.
Major Publications
- Tuffier T. Du rôle de la congestion dans les maladies des voies urinaires. Thèse 1895
- Tuffier T, Hallion. Operations intrathoraciques avec respiration artificielle par insufflation. Comptes rendus hebdomadaires des séances et mémoires de la Société de biologie. 1896; 48: 951-953
- Tuffier T, Hallion. Étude expérimentale sur la chirurgie pulmonaire. Sur les effets circulatoires de la respiration artificielle par insufflation et insufflation soutenue du poumon, Comptes rendus hebdomadaires des séances et mémoires de la Société de biologie. 1896; 48: 1047-1050
- Tuffier T. Chirurgie du poumon. 1897
- Tuffier T. Tuberculose rénale : pathogénie–diagnostic–traitement. 1898
- Tuffier T, Hallion. De la compression rythmée du cœur dans la syncope cardiaque par embolie. Bulletin et Mémoires de la Société de Chirurgie de Paris, 1898; 24: 937-939.
- Tuffier T, Hallion. Syncope chloroformique. Rappel à la vie par la compression rythmée du coeur. Comptes rendus hebdomadaires des séances et mémoires de la Société de biologie. 1898; 50: 988-989
- Tuffier T. Analgésie chirurgicale par l’injection de cocaïne sous l’arachnoïde lombaire. Presse médicale, 15 novembre 1899; 91: 294-295.
- Tuffier T. Musée rétrospectif de la classe 16 : Médecine et chirurgie. 1900
- Tuffier T, Hallion. Expériences sur l’injection sous-arachnoïdienne de cocaïne. Comptes rendus des séances de la Société de biologie et de ses filiales 1900: 895-897
- Tuffier T. Anesthésie medullaire chirurgicale par injection sous-arachnoidienne lombaire de cocaine; technique et results. Semaine médicale 1900; 20: 167–169
- Tuffier T. L’Analgésie chirurgicale par voie rachidienne (injections sous-arachnoïdiennes de cocaïne), technique, résultats, indications. 1901
- Tuffier T. Intervention chirurgicale directe dans un anévrysme de la crosse de l’aorte. Ligature du sac. Bulletins et mémoires de la Société de chirurgie de Paris, 1902; 28: 326-344
- Tuffier T. Technique actuelle de la rachicocaïnisation. Presse médicale, 3 décembre 1902; 97: 1159.
- Tuffier T. La rachicocaïnisation. Paris, 1904
- Tuffier T. Appareil pour la chloroformisation. Bulletins et mémoires de la société de chirurgie de Paris. 1905; 31: 544-546 [Tuffier inhaler]
- Tuffier T. Appareil destiné aux opérations sur les os et à la trépanation crânienne. Bulletins et mémoires de la société de chirurgie de Paris 1905; 31: 1119-1122
- Tuffier T. Titres et travaux scientifiques. 1908
- Tuffier T. Traitement du cancer inopérable 1911
- Tuffier T. Titres et travaux scientifiques. 1913
- Tuffier T. Etat actuel de la chirurgie intra-thoracique: plèvre, poumon, coeur et péricarde, aorte, oesophage. 1914
- Tuffier T. Étude expérimentale sur la chirurgie des valvules du coeur. Bulletin de l’Académie de médecine, 1914 ; 71 : 293-295
References
Biography
- Théodore Tuffier, K.B.E., F.R.C.S. Br Med J. 1929 Nov 9;2(3592):879
- Theodore Tuffier (1857-1929). Ann Med Hist. 1937 May;9(3):284-285.
- Gibson CL. Théodore Tuffier 1857-1929. Ann Surg. 1930 Apr;91(4):636-7.
- Rosney M-A. Théodore Tuffier (1857-1929): chirurgien d’avant-garde. Thèse 1993
- Cousin MT. Un anesthésiste d’avant garde, le chirurgien Théodore Tuffier [A pioneering anesthesiologist, the surgeon Theodore Tuffier]. Ann Chir. 1999;53(5):427-34.
Eponymous terms
Tuffiers line
- Jacoby GW. Lumbar puncture of the subarachnoid space. New York medical journal. 1895; 62: 813-818.
- Jacoby GW. Lumbar puncture of the subarachnoid space. New York medical journal. 1896; 63: 6-12.
- Shiraishi N, Matsumura G. What is the true location of Jacoby’s line? Okajimas Folia Anat Jpn. 2006 Feb;82(4):111-5.
- Walsh JC et al. Variation in position of the L4/5 disc inter-space from the anatomical landmark: review of 450 radiographs and clinical applications. Eur J Orthop Surg Traumatol 2006; 16: 203–206
- Snider KT, Kribs JW, Snider EJ, Degenhardt BF, Bukowski A, Johnson JC. Reliability of Tuffier’s line as an anatomic landmark. Spine (Phila Pa 1976). 2008 Mar 15;33(6):E161-5.
- Horsanalı BÖ, Tekgül ZT, Özkalkanlı MY, Adıbelli ZH, Esen Ö, Duran FY. Radiological Evaluation of the Line Between the Crista Iliaca (Tuffier’s line) in Elderly Patients. Turk J Anaesthesiol Reanim. 2015 Jun;43(3):149-53.
Anaesthetics
- De Rouville G. De l’analgésie chirurgicale par injections de chlorhydrate de cocaïne sous l’arachnoïde lombaire : thèse présentée et publiquement soutenue à la Faculté de médecine de Montpellier le 31 mai 1901
- Cousin MT. Un anesthésiste d’avant garde, le chirurgien Théodore Tuffier [A pioneering anesthesiologist, the surgeon Theodore Tuffier]. Ann Chir. 1999;53(5):427-34.
Chest surgery, cardiac massage, thoracotomy
- Heart and lung surgery. In: Encyclopædia Britannica. 1922; 31: 347-350. 12th Ed
- Barber RF, Wadden JL. Historical aspects of cardiac resuscitation. Am J Surg 1945;70:135.
- Jarcho S. Theodore Tuffier on experimental surgery of heart valves. Am J Cardiol. 1969 Jan;23(1):73-5.
- Bonfils-Roberts EA. The rib spreader: a chapter in the history of thoracic surgery. Chest. 1972 May;61(5):469-74.
- Dobell AR. Theodore Tuffier’s attempt at cardiac resuscitation. Ann Thorac Surg. 1993 Sep;56(3):583-4.
- Ehrhardt JD Jr, Baroutjian A, McKenney M, Elkbuli A. Historical Observations on Clamshell Thoracotomy. World J Surg. 2021 Apr;45(4):1237-1241
Eponym
the person behind the name

BSc MD University of Western Australia. Interested in all things critical care and completing side quests along the way
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |