
![]()
Troubling Lab Strife
aka Oncological Quandary 002
A 30 year-old woman presents with abdominal pain and paraesthesiae. She was diagnosed with CML 2 months previously, and was treated with chemotherapy a month prior to presentation.
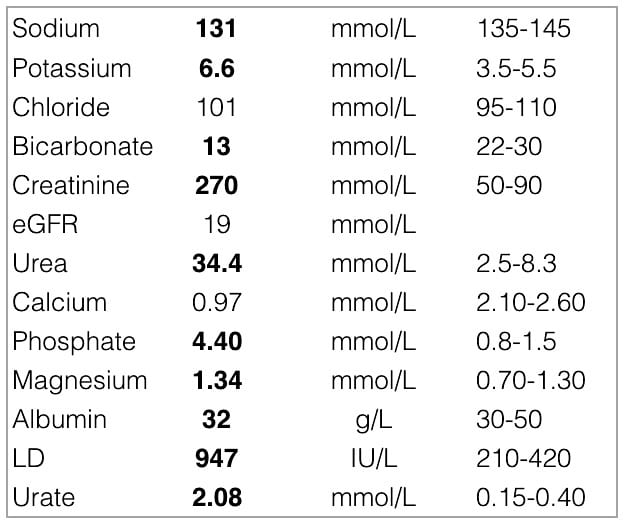
These are her lab results:
Questions
Q1. Describe and interpret the test results.
Answer and interpretation
Description:
- Mild hyponatremia
- Hyperkalaemia
- Hyperphosphataemia
- Hypocalcaemia
- Hyperuricaemia
- High creatinine and urea consistent with renal impairment, with a high urea-to-creatine ratio
- Low HCO3 consistent with metabolic acidosis (lactate is normal)
- High lactate dehydrogenase (LDH)
- Mild hypermagnesaemia and hypoalbuminaemia
Interpretation:
- This constellation of laboratory abnormalities, in a patient receiving chemotherapy for a haematological malignancy, is characteristic of Tumour Lysis Syndrome (TLS).
- The metabolic acidosis is probably due to renal impairment.
- The high urea-creatine ratio suggests a possible pre-renal component — dehydration would be in keeping with the hyponatremia. However, urea is also produced by purine and protein catabolism as occurs in TLS.
- High LDH is a non-specific marker of cell turnover, as occurs in hematological malignancies.
Q2. What is the pathophysiological explanation of the key abnormalities?
Answer and interpretation
The key abnormalities result from the following mechanisms
- Hyperkalaemia is due to rapid expulsion of potassium into the circulation due to cell lysis, and may result in lethal dysrhythmias
- Hyperphosphataemia is due to release of intracellular phosphate due to lysis of tumour cells
- Hypocalcaemia results from a rapid increase in phosphate concentration leading to precipitation of calcium, and may cause tetany and neuromuscular irritability
- Hyperuricaemia is due to increased levels of purine nucleotides into the circulation that are metabolised to uric acid
- Renal failure is multifactorial and is thought to results from a combination of dehydration, uric acid nephropathy and calcium phosphate nephropathy
Lactic acidosis can also be seen in TLS, but is not present in this case.
Q3. What are the risk factors for this condition occurring?
Answer and interpretation
Tumour lysis syndrome is most commonly associated with:
- poorly differentiated lymphomas, e.g. Burkitt’s lymphoma and high-grade non-Hodgkin lymphomas
- leukemias, e.g. acute myeloid leukemia (AML), transformed chronic myeloid leukemia (CML) and acute lymphoblastic leukemia (ALL)
- some fast-growing solid tumours such as hepatocellular carcinoma, hepatoblastoma, testicular cancer, small cell lung cancer, breast cancer and neuroblastoma.
TLS typically occurs about 48-72 hours after chemotherapy is commenced, but spontaneous TLS can also occur (e.g. aggressive lymphomas and leukemias such as Burkitt lymphoma, acute lymphocytic leukemia, large T-cell lymphoma) or it may occur after other cancer treatments (e.g. corticosteroids or radiotherapy).
Hyperphosphatemia tends not to occur in spontaneous TLS, presumably because the phosphate is recycled in the synthesis of new tumour cells (which does not occur when chemotherapy is used).
Pre-existing renal failure may also be a predisposing factor.
Q4. What is your approach to management in this case?
Answer and interpretation
In addition to usual resuscitation measures and supportive care, these are the key management considerations:
- Medical treatment of hyperkalaemia proceeds according to normal guidelines.
- Aggressive rehydration is required (e.g. continue at twice the maintenance rate)
- Phosphate binders can be given.
- Recombinant uric acid oxidase (rasburicase) is used to break down uric acid (contra-indicated in G6PD deficiency).
- Renal replacement therapy is required for refractory cases.
- Administration of calcium can worsen calcium phosphate precipitation. Hypocalcaemia should not treated unless symptomatic, in which administer 10% calcium gluconate.
- Urinary alkalinisation can be used to decrease uric acid precipitation; however, it is generally not required when rasburicase is used and may may precipitate calcium phosphate and xanthine crystals.
References
- CCC — Tumour Lysis Syndrome
- PulmCCM.org — Cancer-Related Medical Emergencies: Tumor Lysis Syndrome
- Cammalleri L, Malaguarnera M. Rasburicase represents a new tool for hyperuricemia in tumor lysis syndrome and in gout. Int J Med Sci. 2007 Mar 2;4(2):83-93. Review. PubMed PMID: 17396159; PubMed Central PMCID: PMC1838823.
- McCurdy MT, Shanholtz CB. Oncologic emergencies. Crit Care Med 2012;40:2212-2222. PubMed PMID: 22584756
CLINICAL CASES
Oncology Quandary
Intensivist in Wellington, New Zealand. Started out in ED, but now feels physically ill whenever he steps foot on the front line. Clinical researcher, kite-surfer | @DogICUma |