
![]()
William Henry Battle
William Henry Battle (1855-1936) was an English surgeon.
Battle was an English surgeon, educator, and clinical innovator, best remembered for his eponymous “Battle sign”—postauricular ecchymosis indicating basilar skull fracture. A meticulous clinician, Battle was a key figure at St. Thomas’ Hospital and the Royal College of Surgeons in the late 19th and early 20th centuries, advancing the understanding of traumatic brain injury, abdominal surgery, and operative techniques.
Educated at St. Thomas’s Medical School, Battle qualified in 1877 and earned his FRCS in 1880. He rapidly established himself as an editor, lecturer, and surgical teacher, and was appointed Hunterian Professor in Surgery and Pathology in 1889. His investigative rigour extended beyond trauma to early innovations in appendicectomy and femoral hernia repair—techniques that still carry his name.
Battle was also an accomplished wartime surgeon, serving as Lieutenant-Colonel in the Royal Army Medical Corps during WWI. Despite the personal loss of his son in 1914, he remained committed to clinical service and teaching, eventually retiring in 1925 after over four decades of practice.
His legacy is that of a careful and consistent surgeon, revered by colleagues and students for his clinical accuracy, thoughtful operations, and teaching clarity. His contributions to trauma signs and abdominal surgery remain part of medical education worldwide.
Biography
- 1855 – Born February 23 in Lincoln, England; son of John Richard Battle, alderman and later mayor of Lincoln.
- 1866–1873 Educated at Lincoln Grammar School (later Lincoln Christ’s Hospital School); excelled in Divinity, History, French, and Drawing.
- 1873 – Entered St. Thomas’ Medical School, London.
- 1877 – Qualified MRCS and LSA; house appointments at St. Thomas’ Hospital.
- 1880 – Became Fellow of the Royal College of Surgeons (FRCS).
- 1880–1886 Surgical Registrar, St. Thomas’ Hospital.
- 1881–1885 Edited St. Thomas’s Hospital Surgical Reports.
- 1883 – Published an early report on postoperative intestinal obstruction.
- 1888 – Assistant Surgeon to East London Hospital for Children and to the Royal Free Hospital; Demonstrator in Practical Surgery at the School of Medicine for Women.
- 1889–1890 – Hunterian Professor in Surgery and Pathology at the Royal College of Surgeons
- 1890 – Delivered lectures to the Royal College of Surgeons describing mastoid ecchymosis in basilar skull fracture (Battle’s sign); published in BMJ.
- 1892 – Appointed Assistant Surgeon at St. Thomas’ Hospital.
- 1892 – Editor of A Mirror of Hospital Practice for The Lancet.
- 1895 – Described vertical incision for appendicectomy (Battle’s incision).
- 1901 – Detailed Battle’s operation for femoral hernia.
- 1903–1911 Edited Saint Thomas’s Hospital reports.
- 1904 – Co-authored The surgery of the diseases of the appendix vermiformis and their complications with Edred Moss Corner (1873-1950)
- 1910 – Delivered annual orations to the Medical Society of London on intra-abdominal trauma.
- 1911 – Published Clinical lectures on the acute abdomen.
- 1914–1918 Served in Royal Army Medical Corps as Major and later Lieutenant-Colonel during WWI at 3rd and 5th London General Hospitals.
- 1914 – Eldest son, Edward, killed in action during the Retreat from Mons.
- 1915 – Extended tenure at St. Thomas’ due to war service.
- 1925 – Retired from hospital practice.
- 1936 – Died February 2 at Horsell Common, Woking, aged 80.
Medical Eponyms
Battle sign (1890)
Battle sign refers to postauricular ecchymosis — bruising over the mastoid process — typically indicative of a basilar skull fracture, particularly involving the posterior cranial fossa. It is a critical clinical finding in trauma assessment and a hallmark sign of serious head injury.
1861 – Sir Prescott Hewett (1812–1891), surgeon to St. George’s Hospital publishes his observation in A System of Surgery:
Extravasation of blood, and consequent discoloration of the skin, appearing in the mastoid region some hours after a severe injury of the head, may lead to the suspicion of a fracture involving the posterior part of the base ; and all the more valuable will this sign will become, if the injury did not bear directly upon this region, and especially if it bore upon the opposite side of the head.
1890 – William Henry Battle (1855–1936) delivers three Hunterian Lectures at the Royal College of Surgeons and later published as Lectures on some points relating to injuries to the head in the Lancet. He systematically describes mastoid ecchymosis in 17 patients and supports his findings through cadaveric injections and anatomical analysis.
He deemed a postauricular ecchymosis to be “a most important indication that the posterior fossa of the skull is the seat of the fracture” and acknowledged the work and description by Hewett previously.
Observations on this subject lead me to the following conclusions with regard to “mastoid ecchymosis.” That it appears, in the first place, in front of the apex of the mastoid process. That it often spreads upwards over the mastoid in a line, slightly curved, and with the con- vexity backwards, its direction being approximately that of the outline of the external ear, from which it is distant half to three-quarters of an inch.
Battle WH, Lancet July 1890
He also described other cardinal signs including otorhinorrhea, subconjunctival haemorrhage and peri-orbital ecchymoses (racoon eyes).
1890s–1900s – The Battle sign becomes widely cited in trauma texts and clinical practice as a key indicator of skull base fracture.
1936 – Battle dies. His contributions to trauma surgery and clinical signs, including Battle sign, are honoured posthumously by colleagues and journals.
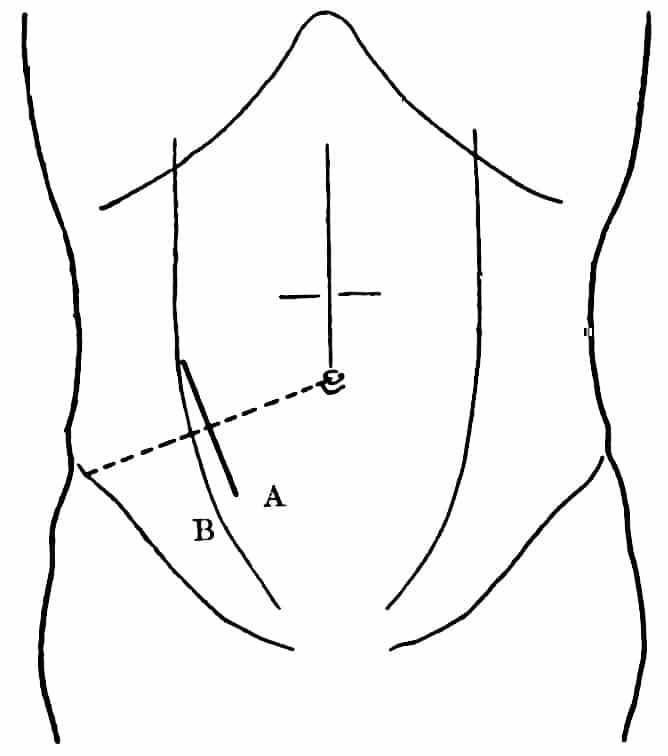
Battle incision (1895)
A vertical abdominal wall incision with medial retraction of the rectus abdominis muscle. Introduced for appendicectomy to reduce trauma and facilitate exposure; still occasionally referenced in surgical texts.– vertical incision of the abdominal wall with temporary retraction of the rectus muscle medially.
Mr. Battle showed a patient, aged 18, on whom he had operated for recurrent appendicitis. He had modified the usual incision in order to prevent the subsequent formation of a hernia, which was so frequent a sequel of this operation. He made the incision 1½ inch to the inside of the linea semilunaris, and divided the aponeurosis of the external oblique with the sheath of the rectus. The rectus muscle was then drawn to the inner side, and the posterior layer of the sheath and transversalis fascia exposed, the inner incision not corresponding to the external. The peritoneum was then divided. He was able to get at the appendix very well through this incision, and the result appeared to him to justify the slightly longer time it took. The layers were sutured from behind forwards, and as the rectus was allowed to return to its place, it thus interposed between the internal and external wounds in the abdomen. The procedure seemed he thought to nold out better hope of avoiding subsequent hernia
Battle operation (1901)
A surgical method for femoral hernia repair, described in The Lancet. Noted for its clarity and effectiveness before modern mesh techniques became standard.
Major Publications
- Battle WH. On obstruction of the inferior vena cava, with cases. St. Thomas’s Hospital Reports 1888; 17
- Battle WH. Three Lectures on Some Points Relating to Injuries to the Head. Br Med J. 1890; 2(1540): 4-10 [Battle sign]
- Battle WH. Lectures on some points relating to injuries to the head. Lancet 1890; 136: 3489: 57–63
- Battle WH. Modified incision for removal of the vermiform appendix. Br Med J 1895; 2: 1360 [Battle incision]
- Battle WH. An undescribed symptom in peritonitis Lancet 1897; 149(3839): 871-872
- Battle WH. A Contribution to the Surgical Treatment of Diseases of the Appendix Vermiformis. Br Med J. 1897 Apr 17;1(1894):965–967
- Battle WH. Abstract of a clinical lecture on femoral hernia. Lancet 1901: 157;4040: 302–305 [Battle operation]
- Battle WH, Corner EM. The surgery of the diseases of the appendix vermiformis and their complications. London, 1904.
- Battle WH. The acute abdomen. London, 1911 (2e 1914)
- Battle WH. Clinical lectures on the acute abdomen. 1912
References
Biography
- William Henry Battle, F.R.C.S. Eng. Lancet 1936; 227(5868): 396-397
- William Henry Battle, F.R.C.S. Br Med J 1936;1:341
- Tubbs RS, Shoja MM, Loukas M. William Henry Battle (1855-1936). J Neurol. 2012 Apr;259(4):790-1.
- Battle, William Henry (1855-1936). Plarr’s Lives of the Fellows
Eponymous terms
- Rao A. William Henry Battle (1855-1936): Battle’s Sign: Bruising Over the Mastoid Process in Fracture of the Base of the Skull. Trauma. 2002;4(2):125-126.
- Tubbs RS, Shoja MM, Loukas M, Oakes WJ, Cohen-Gadol A. William Henry Battle and Battle’s sign: mastoid ecchymosis as an indicator of basilar skull fracture. J Neurosurg. 2010 Jan;112(1):186-8.
- Epperla N, Mazza JJ, Yale SH. A Review of Clinical Signs Related to Ecchymosis. WMJ. 2015 Apr;114(2):61-5.
Eponym
the person behind the name
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |