
![]()
Giovanni Mingazzini

Giovanni Mingazzini (1859-1929) was an Italian neurologist.
Professor Giovanni Mingazzini was known for his extensive contributions to neuroanatomy, particularly with the study of the lenticular nucleus, cerebellum and corpus collosum, as well as the study of aphasia.
Mingazzini performed pioneering studies on aphasia and argued against Pierre Marie’s unitary theory. He advanced the understanding of cerebellar pathways; corpus callosum pathology; putaminal and striatal lesions; aphasia and language pathways; and comparative neuroanatomy of primates. He was also among first in Italy to apply malaria therapy for paralytic dementia.
He was known as “il fondatore della Neurologica Italiana” (the founder of Italian Neurology) a hard-working researcher and teacher and for describing the Mingazzini test and Mingazzini field
Interesting facts: Mingazinni viewed and analysed the brain of the Russian Communist Leader Lenin following the death of the Soviet leader in 1924.
Biography
- 1859 – Born February 15 in Ancona, Italy, to Ferdinando Mingazzini (engineer) and Cesira Franceschelli. Family relocates to Rome; attends secondary school.
- 1877 – Enrolled at the Faculty of Medicine, University of Rome ‘La Sapienza.’
- 1883 – Graduated M.D., University of Rome.
- 1884 – Publishes Manuale di anatomia degli organi nervosi centrali dell’uomo, early manual on neuroanatomy.
- 1884–1886 – Studies neuroanatomy in Munich under Bernhard von Gudden (1824–1886).
- 1885 – Assistant in the Anatomy Institute under Francesco Todaro (1839–1918).
- 1889 – Obtains libera docenza in normal human anatomy.
- 1891 – Appointed anatomical pathologist at Santa Maria della Pietà psychiatric hospital in Rome; establishes advanced neuropathology laboratory.
- 1893 – Obtains libera docenza in neuropathology and psychiatry.
- 1895 – Appointed Professor of Neurology and Psychiatry, University of Rome, succeeding Ezio Sciamanna (1850–1905).
- 1895 – Publishes Il cervello in relazione con i fenomeni psichici.
- 1901 – Describes lenticular hemiparesis (acute putaminal syndrome) — “emiparesi lenticolare di Mingazzini.”
- 1905 – Succeeds Clodomiro Bonfigli (1838–1909) as director of Santa Maria della Pietà psychiatric hospital (until 1924).
- 1906 – Publishes landmark paper on aphasia; disputes Pierre Marie’s views; defines Mingazzini field (“Mingazzinisches Feld”) — subcortical crossroad of language pathways.
- 1907 – Co-founds Italian Society of Neurology (Società Italiana di Neurologia); serves as first Vice-President.
- 1908 – Publishes Lezioni di anatomia clinica dei centri nervosi.
- 1913 – Describes Mingazzini test for latent pyramidal paresis.
- 1914 – Advocates for establishing hospitals for poor neurological patients; contributes to early studies of malaria therapy for neurosyphilis.
- 1921 – After death of Augusto Tamburini (1848–1919), appointed Director of the Clinic of Nervous and Mental Diseases, University of Rome (Clinica delle Malattie Nervose e Mentali).
- 1922 – Publishes Der Balken. Eine anatomische, physiopathologische und klinische Studie on the corpus callosum.
- 1923 – Publishes Le afasie, detailed monograph on aphasia.
- 1924 – Clinica delle Malattie Nervose e Mentali moves to a dedicated building in the university quarter of Rome.
- 1927 – Italian edition editor of Constantin von Economo’s Cytoarchitectonics of the human cerebral cortex.
- 1928 – Publishes on cerebellar, brainstem and language anatomy; comparative studies of apes’ brains.
- 1929 – Dies of a heart attack on December 3 in Rome, aged 70, while still Director of the Clinic.
Medical Eponyms
Mingazzini sign (1913)
A test for subtle hemiparesis, where the participant holds their arms out in front of them with fingers spread. The examiner then observes for lowering of the upper limb.
Barré has been historically cited as being one of the first people to describe this pronator drift and the term “Barré test” is often used to refer to the arm drift test in the detection of a subtle hemiparesis. However, it was Mingazzini (1913) who first described the test – and Jean Alexander Barré who published a demonstration in 1937
Original
English
Il est un autre petit signe de l’hémiparésie organique, et que l’on peut rechercher en étudiant les mouvements du membre supérieur: c’est celui qui consiste en la flexion palmaire précoce de la main lorsque le membre supérieur est placé dans l’attitude du serment. Le procédé employé dans ce cas est le suivant: on demande au sujet d’étendre en avant les bras comme s’il avait à faire le signe du serment, les mains (flg. A) placées au même niveau que l’avant-bras et les doigts écartés. Pour détourner l’attention du sujet, il est bon de lui tenir les yeux fermés. Alors, au bout d’un temps qui peut varier d’une demi-minute à une minute, on voit que le membre affecté de parésie a une tendance à s’abaisser avant l’autre ou à osciller de côté et d’autre: les doigts de la main parétique sont animés de tremblements plus nets ou de légers mouvement d’abduction et d’adduction. Quelquefois, la main seule s’abaisse lentement.
There is another small sign of organic hemiparesis, which can be looked for by studying the movements of the upper limb: it consists of the early palmar flexion of the hand when the upper limb is placed in the attitude of the oath. The procedure used in this case is as follows: the subject is asked to extend his arms forward as if he had to make the sign of the oath, the hands (fig. A) placed at the same level as the forearm and the fingers spread apart. To divert the subject’s attention, it is good to keep his eyes closed. Then, after a time which can vary from half a minute to a minute, we see that the limb affected by paresis has a tendency to lower before the other or to oscillate from side to side: the fingers of the paretic hand are animated by more marked tremors or slight movements of abduction and adduction. Sometimes, the hand alone lowers slowly
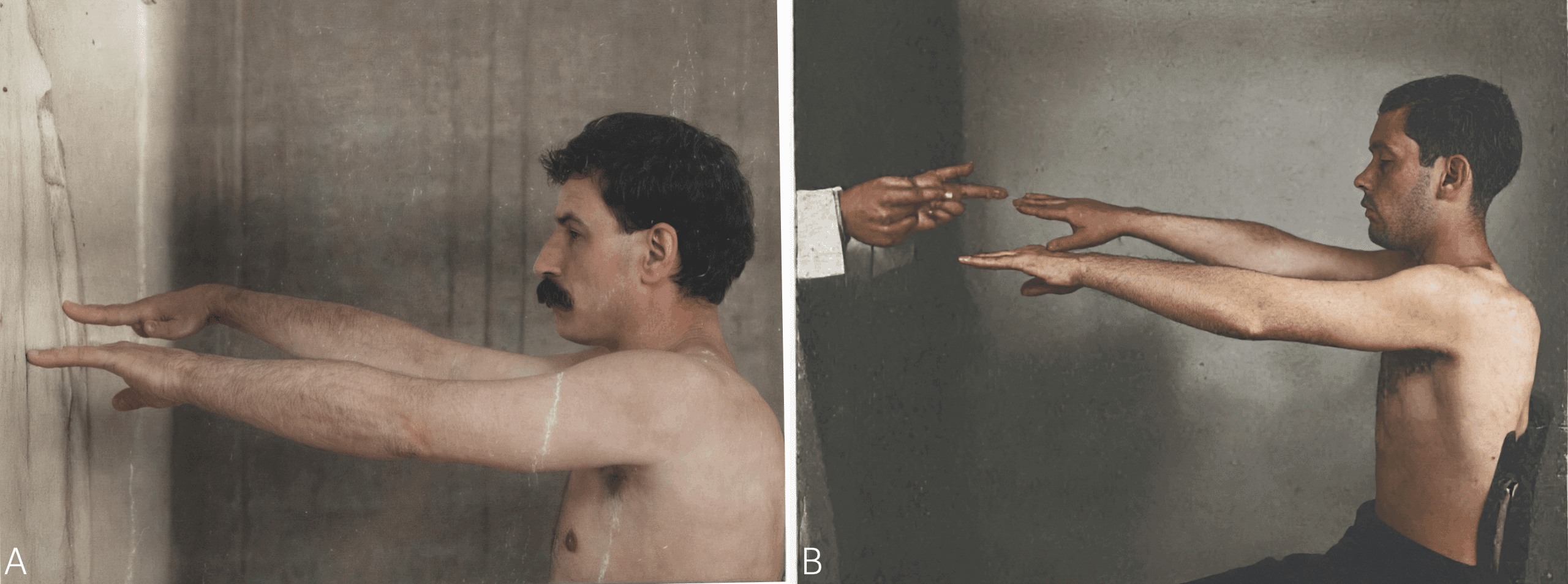
B. Arm test of Mingazzini: from paper by Barré, 1937 [Epreuve du bras de Mingazziai – Le bras gauche s’abaisse verticallment; on peut noter également que l’extension des doigts est moins complète à gauche qu’à droite.]
Mingazzini manoeuvre (1916)
This manoeuvre is sought with the subject in a dorsal position; the thigh is bent at a right angle to the trunk – so it is substantially vertical – while the leg should be held horizontal. On the side of paralysis or pyramidal paresis, the leg lowers and the thigh deflects. Originally described by Mingazzini in 1928 and demonstrated in 1937 by Jean-Alexandre Barré
Fig. 9. Manœuvre de Mingazzini. Positive à droite; — la cuisse se défléchit sur le bassin en même temps que la jambe s’abaisse sur la cuisse.
Original
English
Manœuvre de Mingazzini. Cette manœuvre se cherche sur le sujet en position dorsale ; la cuisse est fléchie à angle droit sur le tronc – elle est donc sensiblement verticale – , tandis que la jambe doit être tenue horizontale. Du côté de la paralysie ou parésie pyramidale, la jambe s’abaisse et la cuisse se défléchit.
Fig. 9. Manœuvre de Mingazzini. Positive à droite; — la cuisse se défléchit sur le bassin en même temps que la jambe s’abaisse sur la cuisse.
Mingazzini maneuver. This maneuver is performed with the subject in a supine position; the thigh is flexed at a right angle to the trunk—it is therefore substantially vertical—while the leg must be held horizontal. On the side of pyramidal paralysis or paresis, the leg is lowered and the thigh is flexed.
Fig. 9. Mingazzini maneuver. Positive on the right; the thigh flexes on the pelvis at the same time as the leg lowers onto the thigh.

Mingazzini field
Term first described by the Swedish internist and pathologist Salomon Eberhard Henschen (1847-1930) in 1925 referring to the area in front of the left lentiform nucleus, where fibers from Broca’s area and the corresponding area in the contralateral hemisphere join – a subcortical area critical in motor aphasia
Original
English
Oft ist jede Besserung der Sprache unmӧglich. Dies ist besonders der Fall nach Zerstӧrung des Mingazzinischen Feldes, das ventral von der zweiten linken Frontalwindung im Mark liegt, wo, nach Angabe von Mingazzini, die Fasern von der rechten F2, durch den Balken zur linken F2 übertreten.
Often any improvement of the language is impossible. This is particularly the case after the destruction of the Mingazzini field, which lies ventrally from the second left frontal gyrus in the medulla, where, according to Mingazzini, the fibres pass from the right F2 [medium frontal gyrus], through the corpus collosum, to the left F2.
Mingazzini’s lenticular hemiplegia
Acute syndrome of the putamen, describing a lesion to the lenticular nucleus which Mingazzini had described in Sulla sintomatologia delle lesioni del nucleo lenticolare in 1901
Major Publications
- Mingazzini G. Il cervello in relazione con i fenomeni psichici; studio sulla morfologia degli emisferi cerebrali dell’uomo. 1895
- Mingazzini G. Osservazioni anatomiche intorno al corpo calloso e ad alcune formazioni che con esso hanno rapporto. 1897
- Mingazzini G. Sulla sintomatologia delle lesioni del nucleo lenticolare. Rivista sperimentale di freniatria e medicina legale delle alienazioni mentali. 1901; 27: 68-93
- Mingazzini G. Beitrag zum Studium der Spondylose rhizomélique. Deutsche Zeitschrift für Nervenheilkunde. 1905; 28(2-4): 176-83. [Bechterew disease (Ankylosing spondylitis)]
- Mingazzini G. Revisione della questione dell’afasia: la terza circonvoluzione frontale sinistra non ha alcuna parte speciale nella funzione del linguaggio. Il policlinico, sezione pratica. 1906; 13: 834- 837, 871–874, 897–905
- Mingazzini G. Les aphasies de conduction en rapport avec la nouvelle théorie de Pierre Marie. L’Encéphale 1908; 3: 1–27
- Mingazzini G. Sur quelques “petits signes” des paresies organiques. Revue Neurologique. 1913; 20(2): 469-473
- Mingazzini G. On aphasia due to atrophy of the cerebral convolutions. Brain 1914; 36: 493–524
- Mingazzini G. Alcuni “piccoli segni” delle paresi organiche. La Riforma Medica. 1914; 27: 78.
- Mingazzini G. Der Balken : eine anatomische, physiopathologische und klinische Studie. 1922
References
Biography
- Fumarola G. Giovanni Mingazzini. Il Policlinico: Sezione Pratica. 1929; 36(2): 1900-1902
- Obituary. Giovanni Mingazzini (1859-1929). Arch Neur Psych. 1930; 23(4): 798-799.
- Brigo F, Nardone R. Giovanni Mingazzini (1859-1929) and his opposition to Pierre Marie’s conception of motor aphasia. Neurol Sci. 2020 Oct;41(10):2973-2976.
- Triarhou LC. Giovanni Mingazzini (1859-1929). J Neurol. 2021 Apr;268(4):1558-1559.
- Rigo GS, Armocida G. MINGAZZINI, Giovanni. Biographical Dictionary of Italians. 2010; Volume 74
Eponymous terms
- Henschen SE. Über die funktion der rechten hirnhemisphäre im verhältnis zu der linken, in bezug auf sprache, musik und rechnen. Zeitschrift für die gesamte Neurologie und Psychiatrie, 1926; 100(1): 1-16
- Barré JA. Le syndrome pyramidale deficitaire. Revue Neurologique. 1937; 67(1): 1-40
- Koehler PJ, Bruyn GW, Pearce JMS. Neurological Eponyms. Oxford University Press 2000; 119-126
- Hirose G. [The Barrés test and Mingazzini test -Importance of the original paper by Giovanni Mingazzini]. Rinsho Shinkeigaku. 2015;55(7):455-8
Eponym
the person behind the name
Physician in training. German translator and lover of medical history.