
![]()
Józef Dietl

Józef Dietl (1804–1878) was a Polish physician, politician, professor and rector
Dietl is remembered as a pioneer in public health, a reformer of medical education, a devoted public servant, and a devout Polish patriot.
Instigator of clinical trials and formative evidence based medicine to overhaul medical dogma. He conducted trials, provided statistical evidence and expressed his doubts about the forms of therapy common at the time so vehemently that he has been termed the founder of “therapeutic nihilism.”
He also contributed to reform of the educational system, and to bringing order to the badly neglected city of Kraków. He be longed to the New Vienna School of Medicine along with the ‘Dreigestirn‘ of Carl von Rokitansky (1804-1878); Ferdinand von Hebra (1816–1880) and Joseph Škoda (1805–1881). The old school carried on therapy before engaging in research, the new school began researching in order to be able to undertake therapy. The New Vienna School was trying to move medicine along the lines of rational and scientific study.
Dietl claimed that acquaintance with the human body, based on the natural sciences, had to be a pre-condition for clinical medicine. In his work “Anatomische Klinik der Gehirnkrankheiten” (An anatomical analysis of brain disturbances), Dietl described the role of pathological anatomy in clinical research and that morbid anatomy was the fundamental doctrine of medicine.
He was a pioneer of balneology and considered to be the father of balneology in Poland
Biography
- Born January 24, 1804 Podbużu
- 1841 – chief physician in the Department of Internal Medicine, Wieden hospital in the outskirts of Vienna
- 1845 – Article ‘Praktische Wahrnehmungen nach den Ergebnissen der vorjährigen Epidemie im Wiener Polizeibezirke Wieden‘ outlined the major ideas of the pathologic and therapeutic points of view of the New Vienna School of Medicine known as the ‘Manifesto of the Vienna School’
- 1848 – director of Wieden hospital
- 1850-1853 – traveled extensively within Europe and beyond, funded by the Austrian government, to review and evaluate hospital organization and treatment methods culminating in his publication of “Kritische Darstellung europäischer Krankenhauser” (Critical description of European hospitals), the first significant German-language work in the field of hospital hygiene
- 1854-1858 promoted the study and development of balneotherapy and climatotherapy and published his ‘Balneologische Reiseskizzen‘ (Balneological travel notes) and ‘Uwagi nad zdrojowiskami krajowymi ze względu na ich skuteczność, zastosowanie i urządzenie‘ (Comments on polish health resorts concerning their effectiveness, use, and equipment)
- 1851-1865 head of the Department of Pathology and Specific Therapy and the Medical Clinic, Kraków. Clinical educator and the first in Kraków to teach percussion and auscultation and the use of the pleximeter and stethoscope.
- 1862 – led an education campaign against the Polish plait – a mass of matted hair, known as plica polonica (trichoma). Contrary to popular opinion he published ‘Plica. Report of a Commission Established by the Kraków Scientific Society to Investigate the Condition Known as Plica Disease‘
- 1861 – rector of Jagiellonian University (Uniwersytetu Jagiellońskiego, Kraków)
- 1865 – Dietl was ‘retired‘ from medicine as a result of anti-Austrian politics
- 1866-1874 mayor of Kraków
- Died January 18, 1878 in Kraków
- Honours: Franz-Joseph-Orden (as Professor); Orden der Eisernen Krone (as mayor); Gregoriusorden (Nuntius in Krakau)
Original
English
So lange die Medizin eine Kunst ist, wird sie keine Wissenschaft sein; so lange es glückliche Ärzte gibt, solange gibt es keine wissenschaftlichen Ärzte. Nach der Summe seines Wissens und nicht nach dem Erfolge seiner Kuren muß der Arzt beurteilt werden. Denn im Wissen und nicht im Handeln liegt seine Kraft
Dietl 1851
As long as medicine is an art, it will not be a science; as long as there are successful physicians, there will be no scientific physicians. A physician must be judged by the sum of his knowledge, not by the success of his treatments. For his strength lies in knowledge, not in action
Dietl 1851 – paradoxes forming the ethos of therapeutic nihilism at the New Vienna School
Medical Eponyms
Dietl’s crisis (1864)
In modern parlance, Dietl’s crisis, is used to define episodic, crampy upper abdominal pain, nausea and vomiting associated with ureteropelvic junction obstruction (UPJO).
This is probably the best current use of the eponymous term…as the real eponymic history is less clear
In the days before radiological imaging, physicians relied on clinical observation and autopsy to enhance pathological understanding. Dietl published his experiences in Kraków between 1858 and 1862 regarding a constellation of abdominal symptoms which he proposed were associated with the abnormal descent of a kidney. Unfortunately none of his patients died and without necropsy he was unable to determine the pathological cause for the symptoms. Instead he postulated ischaemic strangulation of a wandering kidney (nephroptosis); or torsion of the renal pelvis with ureteral obstruction to be the cause…stimulating myriad operative interventions to avert the newly described abdominal catastrophe.
1864 – Dietl reported nine cases of movable kidney ‘Wandernde nieren und deren einklemmung‘ in the Wiener medicinische Wochenschrift. Each presented with right upper quadrant and right flank pain, which radiated periumbically or to lumber, genital, or right subscapular areas. Nausea, vomiting, indigestion, weakness, and anxiety were common; fever and diminished urinary output less so. Urine was clear in three instances and highly coloured in one; the presence of blood was not mentioned. In four there were also attacks of nausea and vomiting, with great pain, swelling, and tenderness of the affected kidney. Manual replacement was frequently efficacious, although several patients suffered recurrences. Eventually each subject appeared to respond to quinine, iron, and the application of an abdominal binder. Followup was limited, and Dietl rather apologetically reported that he could say little about morbid anatomy because no patients had died
Original
English
Nachdem ich nun bemüht war in gedrängter Kürze ein klinisches Bild von dieser in unserem Lande so häufig vor kommenden anormalen Lage der Nieren zu geben, muss ich nur bedauern dasselbe durch nekroskopische Darstellungen nicht ergänzen und illustriren zu können, da von allen von mir beobachteten Fällen dieser Art kein einziger zur Sektion gelangte. Es muss künftigen Beobachtungen Vorbehalten bleiben, ob nicht manche von dem Hypochondrium ausgehende, an der hinteren Bauchwand dahinziehende über Gekröse und Netz sich verbreitende Peritonitis, ja vielleicht manche Paranephritis zu nächst aus der Einklemmung einer beweglichen Niere her vorgehe.
Having endeavoured to provide a brief clinical picture of this abnormal position of the kidneys, which is so common in our country, I must only regret not being able to supplement and illustrate it with necroscopic images, since not a single one of all the cases of this type I have observed has been autopsied. It must be left to future observations to determine whether some peritonitis originating in the hypochondrium, spreading along the posterior abdominal wall via the mesentery and omentum, and perhaps even some paranephritis, may not initially result from the entrapment of a mobile kidney.
Osler continued the eponymic history attributing the term ‘Dietl’s Crises‘ in his ‘Principles and Practices of Medicine’ (eight editions 1892-1918) and other publications
(b) Dietl’s Crises in Movable Kidney – Remarkable attacks of pain occur in connection with movable kidney, to which attention was first called by Dietl. A knowledge of the existence of these renal crises, as they have been termed, is very important, and as they form a very striking feature in certain cases of movable kidney…Dietl was doubtful about the pathology of the condition, but from the title of the paper, “Wandering kidneys and their entrapment“, it is evident that he regarded it as a strangulation caused probably by a twist in the vessels.
However nephroptosis and the ischaemic kidney as the pathological cause of the symptom constellation waned through the 1900s being replaced by conditions such as renal colic and pelviureteric junction obsctruction
For instance, it is well recognized today the classical description of renal colic, the so called Dietl’s crisis, of pain sharp and cutting, referred downward from the kidney-region along the course of the ureter to either the testicle or vulva…
…and by the 1990s it was almost gone. Dietl’s crisis had almost disappeared – banished to the eponymic lake of misunderstanding and misinterpretation…
but no…
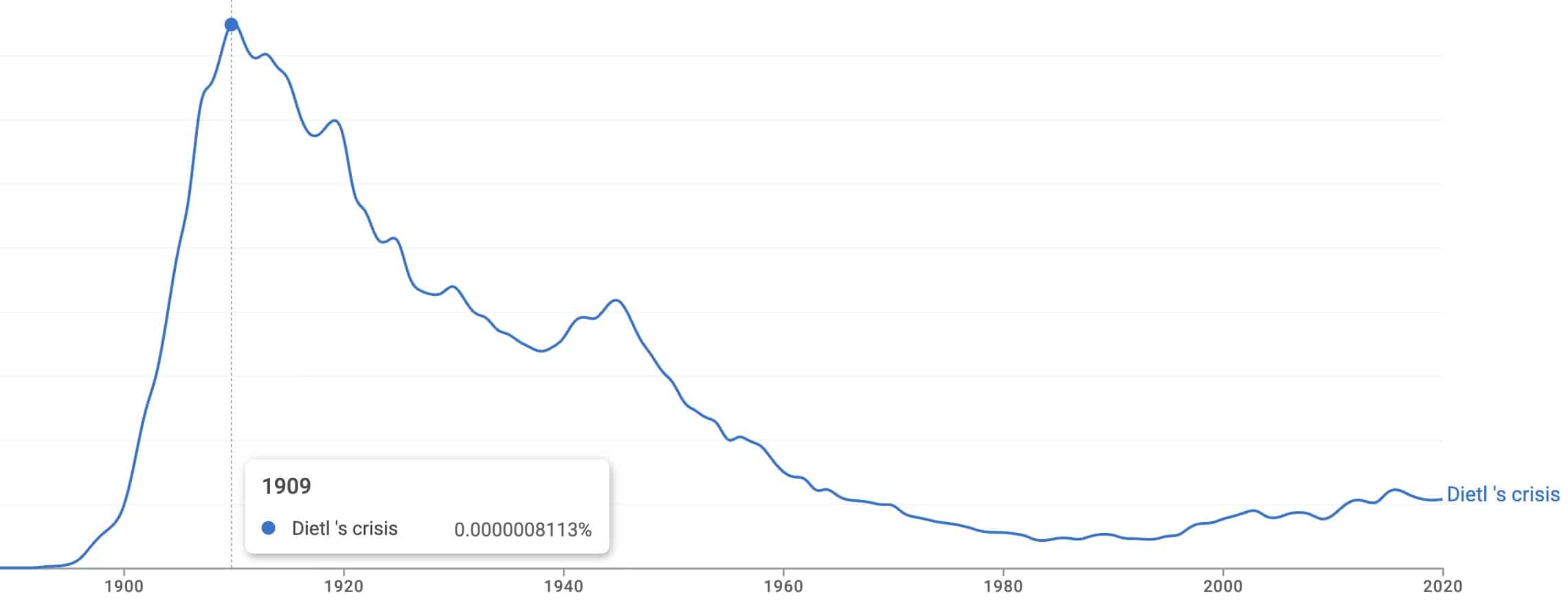
…Dietl’s crisis (defined as ureteropelvic junction obstruction (UPJO) and pelviureteric (PUJ) obstruction)…is back baby. And all the cool kids are writing about it [Austin Powers paediatric reference]
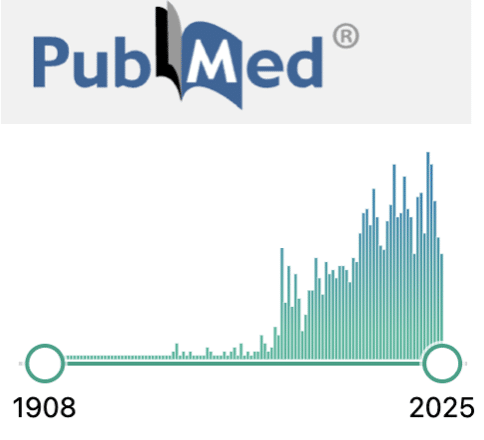
2021 – Dietl’s crisis is described as episodic, crampy upper abdominal pain, nausea and vomiting associated with intermittent renal pelvi-ureteric junction (PUJ) obstruction. A child with this crisis often has a delay in diagnosis, with the clinical entity being underdiagnosed. Dietl’s crisis is one of the curable causes of intermittent abdominal pain [Maddileti et al]
2022 – Ureteropelvic junction obstruction: Older children may present with severe intermittent flank or abdominal pain associated with nausea and vomiting, known as Dietl’s crisis. MAG-3 imaging confirms the diagnosis [Bailey And Love 28e]
2024 – Dietl’s crisis is a commonly missed diagnosis in the pediatric population that presents with intermittent episodes of pain and vomiting. It can be readily diagnosed at the bedside by the emergency physician (EP) through the employment of point of care ultrasound (POCUS). [Thom et al]
Clinical trial and evidence based medicine
The treatment of pneumonia
In the 1840s it was still believed that pneumonia depended on an imbalance between the bodily fluids. Exactly which fluids were out of balance was contentious – some physicians recommended bloodletting whereas others favoured the administration of an emetic.
1849, Dietl reported an investigation in which he had compared three groups of pneumonia patients. One group had received bloodletting, the second an emetic, and the third received general care but no specific treatment. He compared mortality among those who had received bloodletting (20.4%), an emetic (20.7%), and no specific treatment (7.4%).
Dietl’s publication was received negatively at first. His critics claimed that since disease and treatment are highly individual issues, they cannot be settled with statistics. They defended the idea of medicine as an intuitive art that goes beyond what can be determined by scientific method. However, Dietl was successful in the end and the major medical textbooks advised against bloodletting of pneumonia patients by the late 1870s.
Original
English
Aber selbst da, wo es dem Arzte wegen des regelmässigen Verlaufes der Pneumonie nicht gestattet ist, thatkräftig in das Heilgeschäft einzugreifen, ist doch sein Nutzen für den Kranken vom höchsten Belange! Ist es doch der Arzt, der die Natur desUebels erkennt, der die entsprechenden diätetischen Mittel anordnet und die schädlichen Einflüsse hintanhält, der den wahrscheinlichen Ausgang der Krankheit vorhersagt, der das Erlöschen des Krankheitsprocesses ausmittelt , der die Verhaltungsregeln für die Zukunft vorschreibt, der durch weise Rathschläge den Genesenen vor künftigen Gefahren schützt und bewahrt ! Ist die Wirksamkeit des Arztes darum minder wohlthätig, weil sie ein fache i ist? Ist der Arzt darum weniger werth, weil er mit geringen Mitteln grosse Erfolge zu erzielen versteht? Gerade die Einfachheit der Therapie slämpelt den Arzt zum grössten, unbestreitbaren Wohlthäter des Leidenden, und die Medicin wird erst dann ihren vollen Segen über die Menschheit verbreiten, wenn sie mehr auf vernünftigen Rathschlägen, denn auf complicirten Arzneiformeln beruhen wird.
Wir glauben daher, dass dem auf die Lanzette verzichtenden Arzte noch immer ein sehr weites Feld für seineWirksamkeit übrig bleibt, das er um so ehrenvoller behaupten wird, als er mit erlaubten Waffen der Nothvvehre kämpft, die immer nur den Feind treffen , ohne je den Freund zu verletzen.
But even where the doctor is not permitted to actively intervene in the treatment process due to the regular course of pneumonia, his benefit to the patient is still of the utmost importance! After all, it is the doctor who recognizes the nature of the illness, who prescribes the appropriate dietary remedies and counteracts harmful influences, who predicts the likely outcome of the disease, who determines the extinction of the disease process, who prescribes rules of conduct for the future, who protects and preserves the recovered from future dangers through wise advice! Is the doctor’s activity any less beneficial because it is a simple i? Is the doctor of less value because he knows how to achieve great results with limited means? Precisely the simplicity of therapy makes the physician the greatest, undeniable benefactor of the suffering, and medicine will only spread its full blessings upon humanity when it is based more on sound advice than on complicated medicinal formulas.
We therefore believe that the physician who foregoes the lancet still has a very broad field of effectiveness left, which he will assert all the more honorably since he fights with legitimate weapons of emergency, which always strike only the enemy, never injuring the friend.
Major Publications
- Dietl J. Einige Worte über die Zuverlässigkeit der Heilwissenschaft zur besonderen Beherzigung für nicht Ärzte. Wien 1829
- Dietl J. Praktische Wahrnehmungen nach den Ergebnissen der vorjährigen Epidemie im Wiener Polizeibezirke Wieden. [Practical observations based on the results of the previous-year’s epidemic in Wieden]. 1845
- Dietl J. Anatomische Klinik der Gehirnkrankheiten. Wien 1846
- Dietl J. Der Aderlass in der Lungenentzündung: klinisch und physiologisch erörtert. [Bloodletting in pneumonia from clinical and physiological stand points]. Wien 1849
- Dietl J. Kritische Darstellung europaeischer Krankenhäuser nach eigenen Reisebeobachtungen. 1853
- Pamiętnik Towarzystwa Lekarskiego Warszawskiego
- Dietl J. Bemerkungen über die einheimischen Kurorte im Hinblick auf Ihre Wirkung. Kraków, 1858: S1–363
- Dietl J. We˛druja˛ca s´ledziona. Zapalenie otrzewnej. S´mierc´(Wandering Spleen. Peritonitis. Death). Prz Lek 1863; 2: 98–100
- Dietl J. Merki wedriyace i ich uweizquienic. Przegl Lek 1864; 3: 225-27, 233-35, 242-43,.
- Dietl J. Wandernde nieren und deren einklemmung. Wiener medicinische Wochenschrift. 1864; 14 (36, 37, 38): 563-66, 579, 593-95 [PDF combined]
References
Biography
- Bichoński R. Józef Dietl reformator nauk medycznych [Jozef Dietl–reformer of medical sciences]. Arch Hist Med (Warsz). 1978;41(2):147-50.
- Kucharz E. The life and achievements of Joseph Dietl. Clio Med. 1981 Sep;16(1):25-35
- Zajaczkowski T. Joseph Dietl (1804-1878). Reformer der Medizin und sein Beitrag für die Urologie [Joseph Dietl (1804-1878). Reformer of medicine and his contributions to urology]. Urologe A. 2006 Jan;45(1):85-94.
Eponymous terms
- Hightower JM. Dietl’s crisis revisited–the enigma of nephroptosis. West J Med. 1995 May;162(5):471.
- Mergener K, Weinerth JL, Baillie J. Dietl’s crisis: a syndrome of episodic abdominal pain of urologic origin that may present to a gastroenterologist. Am J Gastroenterol. 1997 Dec;92(12):2289-91.
- Magowska A. Wandering spleen: a medical enigma, its natural history and rationalization. World J Surg. 2013 Mar;37(3):545-50.
- Fu K, Jia W, Fu W, Zhang LY, Hu JH, Zhao Z, Liu G, Zhu SB, Liu GC. Abdominal pain as a result of intermittent hydronephrosis. Eur Rev Med Pharmacol Sci. 2018 May;22(10):3126-3129.
- Maddileti V, Gazula S, Dantala P, Srinivas M. Dietl’s crisis: an under appreciated clinical entity in the paediatric population. BMJ Case Rep. 2021 Aug 16;14(8):e244943.
- Thom C, Larsen M, Kongkatong M, Ottenhoff J, Moak J. It’s Not Cyclic Vomiting Syndrome Until Dietl’s is Ruled Out: A Case for Point of Care Renal Ultrasound. J Emerg Med. 2024 Oct;67(4):e346-e350
Eponym
the person behind the name