
![]()
Airway Case 001
78 year old male is transferred to hospital with lethargy, and altered mental status and persistent vomiting. Of note he suffered an ischaemic stroke 4 weeks prior with residual right sided hemiparesis and dysarthria.
His medical history includes the diagnoses of Parkinson’s Disease, hyperlipidaemia and hypertension and is currently taking aspirin and clopidogrel. Per EMS, on their arrival he had a GCS of 9, and emesis x3 en route.
On examination his GCS is 7 and he is actively vomiting. The team decides to proceed with intubation for airway protection.
Despite careful intubation technique, a chest x-ray done after admission shows bilateral patchy infiltrates in the bilateral lower lobes.
Video laryngoscopy
- VL demonstrates emesis/stomach contents coming from the airway that requires suction.
- The operator leads with suction catheter, and park the suction in the oesophagus to maintain a clear field of view.
- The laryngoscope is inserted slightly deep over the epiglottis but quickly corrected to engage the vallecula and an off centre, grade IIa view is attained
- The bougie is directed with some difficulty toward the vocal folds and glottis. After passing the bougie, the endotracheal (ET) tube is passed smoothly over the bougie.
- The view is lost as the bougie is being removed from the ET tube.
Airway Management Learning points
Airway contamination
- Leading with suction will allow a better view and avoid camera contamination if using video laryngoscopy, as described in the “SALAD technique.” [1]
- Furthermore, “seating” the suction in the proximal oesophagus allows for continuous drainage of airway contamination while freeing up the operators dominant hand to intubate.
Issue passing your equipment? Pivot!
- Blade: The proceduralist initially inserts the laryngoscope blade too deep and over the epiglottis. They quickly recognize this, remove the blade slightly and seat the blade in the vallecula
- Bougie: The intubator had difficulty directing the bougie towards the vocal folds and through the glottis in the setting of a grade IIa view that was off midline. As a result, it took multiple attempts to place the tip of the bougie into the glottis. To mitigate this, reposition the laryngoscope in the vallecula to place the view in the midline.
- Catheter: The suction catheter exits the mouth to the right of the laryngoscope blade and is in the way of the bougie entering from the right. When parking suction in a contaminated airway, move the catheter to the left of the blade to allow more room and better bougie manoeuvrability.
Follow through:
- The intubator did not maintain the obtained view before removing the bougie from the ET tube.
- Therefore, tube presence in trachea and evidence of the balloon passing the cords cannot be confirmed – this is an error of tube delivery. [2]
Clinical Learning Points: Aspiration
Aspiration pneumonitis represents chemical injury of the lungs by acidic gastric contents, whereas aspiration pneumonia is an infectious process secondary to pulmonary exposure bacteria
Prophylactic antibiotics are not routinely indicated for aspiration pneumonitis; however empiric antibiotics may be appropriate for select patient populations (shock, requiring intubation) [3, 4]
Selection of antibiotics for aspiration pneumonia depends on multiple factors:
- Patients with severe illness, healthcare-associated aspiration, or other risk factors for resistant organisms may require broader coverage than typical CAP treatment [4, 6, 7]
- Routine anaerobic coverage is not recommended unless poor dental health or necrotizing pneumonia is present [4, 6]
Corticosteroids are not recommended for routine use in aspiration pneumonitis, with data showing no benefit and some potential harm [3, 4, 5]
Appendix
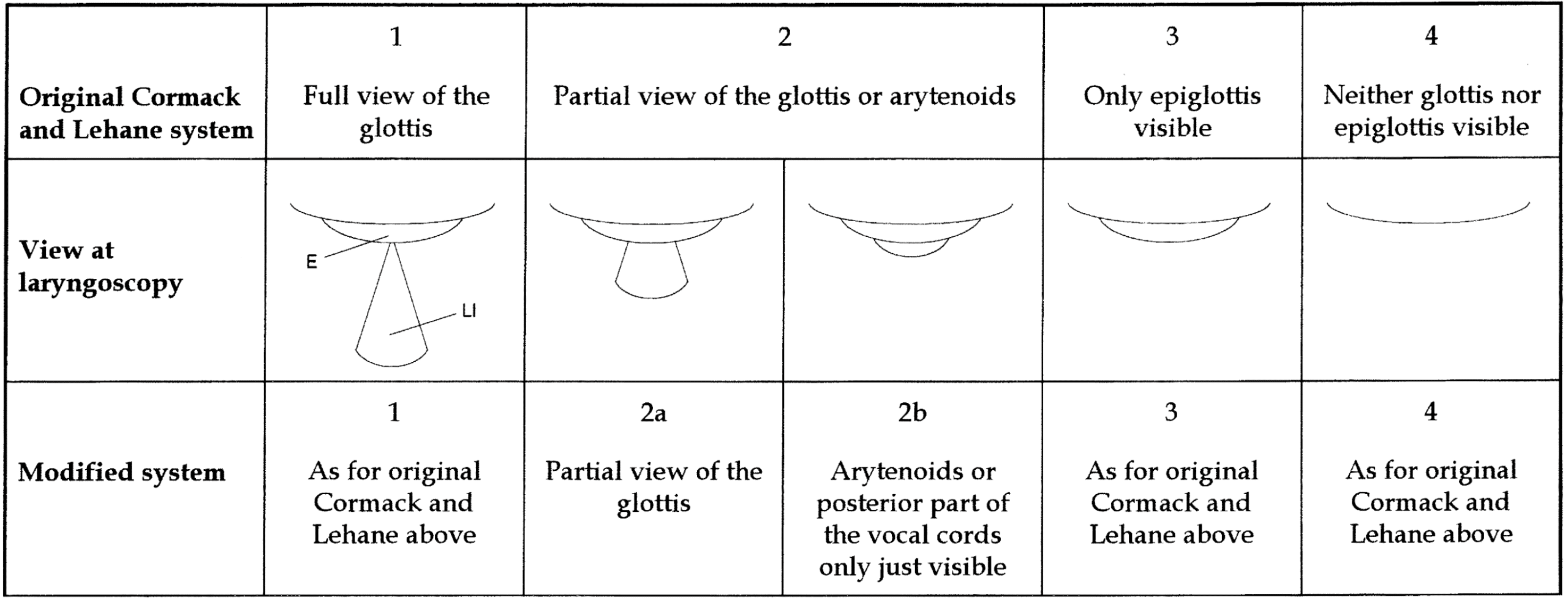
Grading of direct laryngoscopy. Yentis and Lee, 1998
References
- DuCanto J, Serrano KD, Thompson RJ. Novel Airway Training Tool that Simulates Vomiting: Suction-Assisted Laryngoscopy Assisted Decontamination (SALAD) System. West J Emerg Med. 2017 Jan;18(1):117-120.
- Weingart SD, Barnicle RN, Janke A, Bhagwan SD, Tanzi M, McKenna PJ, Bracey A; Resuscitationists Research Group. A taxonomy of key performance errors for emergency intubation. Am J Emerg Med. 2023 Nov;73:137-144.
- Marik PE. Aspiration pneumonitis and aspiration pneumonia. N Engl J Med. 2001 Mar 1;344(9):665-71.
- Mandell LA, Niederman MS. Aspiration Pneumonia. N Engl J Med. 2019 Feb 14;380(7):651-663.
- Moore FA. Treatment of aspiration in intensive care unit patients. JPEN J Parenter Enteral Nutr. 2002 Nov-Dec;26(6 Suppl):S69-74; discussion S74.
- Makhnevich A, Feldhamer KH, Kast CL, Sinvani L. Aspiration Pneumonia in Older Adults. J Hosp Med. 2019 Jul 1;14(7):429-435.
- Zaragoza R, Vidal-Cortés P, Aguilar G, Borges M, Diaz E, Ferrer R, Maseda E, Nieto M, Nuvials FX, Ramirez P, Rodriguez A, Soriano C, Veganzones J, Martín-Loeches I. Update of the treatment of nosocomial pneumonia in the ICU. Crit Care. 2020 Jun 29;24(1):38
- Yentis SM, Lee DJ. Evaluation of an improved scoring system for the grading of direct laryngoscopy. Anaesthesia. 1998 Nov;53(11):1041-4.

Gabriella Sansaricq MD, The Warren Alpert Medical School of Brown University. Emergency Medicine Resident Physician at at Mount Sinai Hospital, New York. Interested in healthcare administration and operations, critical care, community medicine, medical innovation and informatics and physician wellness.

Dr. Tim Friedmann, MD is an Assistant Professor in the Department of Emergency Medicine at the Icahn School of Medicine at Mount Sinai. He is an Assistant Program Director for the residency program and works clinically at Mount Sinai Hospital and Elmhurst Hospital | Sinai EM |