
![]()
Arthur Barker
Arthur Edward James Barker (1850-1916) was an Irish-born British surgeon and pioneer of local and spinal analgesia
Educated in Dublin and Bonn, Barker brought a strong German surgical influence to British practice, particularly in operative precision, asepsis, and experimental observation. He was appointed Assistant Surgeon to University College Hospital at the young age of 25, later becoming full surgeon and Professor of the Principles and Practice of Surgery and Clinical Surgery.
As a general surgeon his work ranged across abdominal, neurological, otological, orthopaedic, and reconstructive surgery. Achievements included early successful gastroenterostomy for pyloric cancer, operative treatment of acute intussusception, drainage of intracranial abscess secondary to middle-ear infection, renal surgery, patella fracture fixation, psoas abscess treatment, surgical instrument design, and work on leukoplakia as a precursor of tongue epithelioma. Barker also helped move British surgery from Listerian antisepsis toward a more modern aseptic ritual, emphasising heat sterilisation, theatre discipline, “no-touch” technique, and avoidance of contamination from hands, clothing, dressings, and breath.
Barker was one of the earliest British surgeons to investigate and refine local infiltration analgesia. He published practical papers on dilute local anaesthetic solutions, especially β-eucaine, and later β-eucaine with adrenaline.
In spinal anaesthesia he studied drug density, spinal curvature, patient position, and the effect of gravity, needle placement, and the mechanics of reliable intrathecal injection. He recognised that CSF could appear at the needle hub even when the terminal opening was only partly within the dural sac, allowing injected anaesthetic to escape partly into the extradural space. His solution was a projecting blunt inner cannula passed through the spinal needle to deliver anaesthetic beyond the needle tip.
Biographical Timeline
- Born May 10, 1850 in Dublin, son of Dr William Barker and Margaret Houghton
- 1870 – Qualified LRCSI, Royal College of Surgeons in Ireland. Travelled to Bonn for further surgical training, where he gained fluency in German and French.
- 1874 – Published an English translation of Heinrich Frey’s Histologie und Histochemie des Menschen, an important German histology text.
- 1875 – Returned to Dublin and was appointed surgeon to the City of Dublin Hospital and demonstrator of anatomy at the Royal College of Surgeons in Ireland.
- 1876 – Moved to London and was appointed Assistant Surgeon to University College Hospital. Awarded FRCSI.
- 1880 – Awarded FRCS England ad eundem.
- 1880 – Married Emilie Blanche Delmege of Rathkeale, County Limerick. They had two sons and four daughters.
- 1885 – Appointed full surgeon to University College Hospital, where he remained on the active staff until 1915.
- 1886 – Performed the first successful gastroenterostomy for malignant disease in Britain, for carcinoma of the pylorus; the patient survived for just over one year.
- 1886–1889 – Advanced operative treatment of otological and intracranial infection, including successful drainage of a temporosphenoidal cerebral abscess secondary to middle ear infection. His Hunterian lectures in 1889 addressed intracranial inflammation starting in the temporal bone.
- 1887 – Published A Short Manual of Surgical Operations, self-illustrated
- 1893 – Elected Professor of the Principles and Practice of Surgery and Clinical Surgery at University College Hospital Medical School.
- 1899–1904 – Published on local infiltration analgesia, becoming one of the earliest British surgeons to adopt and refine local analgesic techniques.
- 1906 – Published clinical lecture on “The hands of surgeons and assistants in operations”, reflecting his major interest in asepsis, theatre discipline, and surgical infection prevention.
- 1907 – Published his first report on clinical experiences with spinal analgesia in 100 cases in the British Medical Journal.
- 1908 – Published second and third reports on spinal analgesia
- 1909 – Addressed spinal analgesia at the British Medical Association meeting in Belfast.
- 1914–1916 – Served during the First World War as a Colonel in the Army Medical Service and Royal Army Medical Corps, with service at Netley, then Malta, and finally Salonika.
- Died on April 8, 1916 at Salonika, from pneumonia.
Key Medical Contributions
Barker and spinal analgesia
Barker was not the first British surgeon to use spinal analgesia, but he was one of the most important figures in making the technique acceptable in British surgical practice. Barker was a pioneer who studied intradural spinal analgesia, used it in his own surgical practice, investigated its spread, and helped convince contemporaries that it could be safe and effective for selected operations.
In 1907, Barker published his clinical experiences with spinal analgesia in 100 cases, followed by two further reports in 1908 bringing his published experience to 300 cases. He studied clinical results, drug density, spinal curvature, patient position, asepsis, puncture technique, and the mechanical problem of reliable intrathecal injection.
The “orifice straddling the dura”
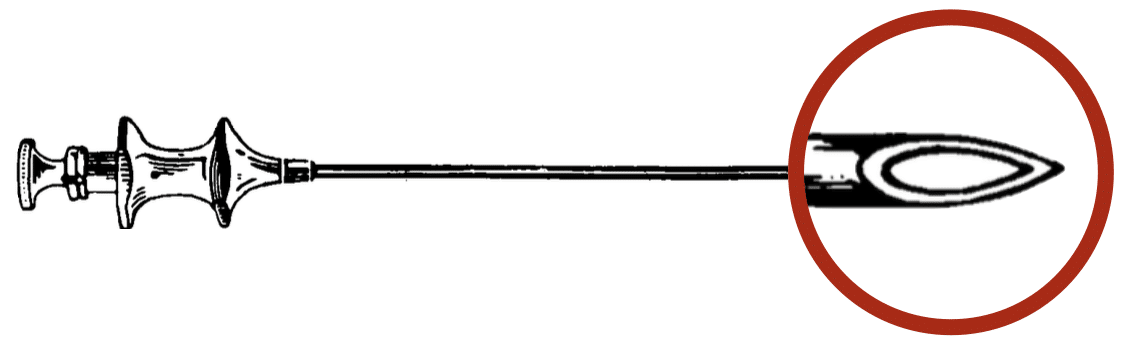
Barker identified a key failure in early spinal analgesia (Figure 1), that CSF might appear at the hub even when the terminal opening of the needle was only partly within the dural sac. Injected anaesthetic could therefore be divided between the subarachnoid and extradural spaces. To solve this, he developed a slender blunt cannula passed through the hollow spinal needle after dural puncture, projecting about 1 mm beyond the needle tip. This delivered the anaesthetic agent beyond the needle opening and into the CSF.
Barker’s apparatus was a purpose-built spinal injection system rather than a single needle (Figure 2). It included a Bier-type hollow puncture needle, a close-fitting stylet, a projecting blunt cannula for injection, and a 2 mL Record syringe. The needle’s hollowed-out point was intended to remain sharp without creating an excessively long terminal opening, while the blunt cannula ensured that the injectate was delivered beyond the needle tip and into the dural sac.
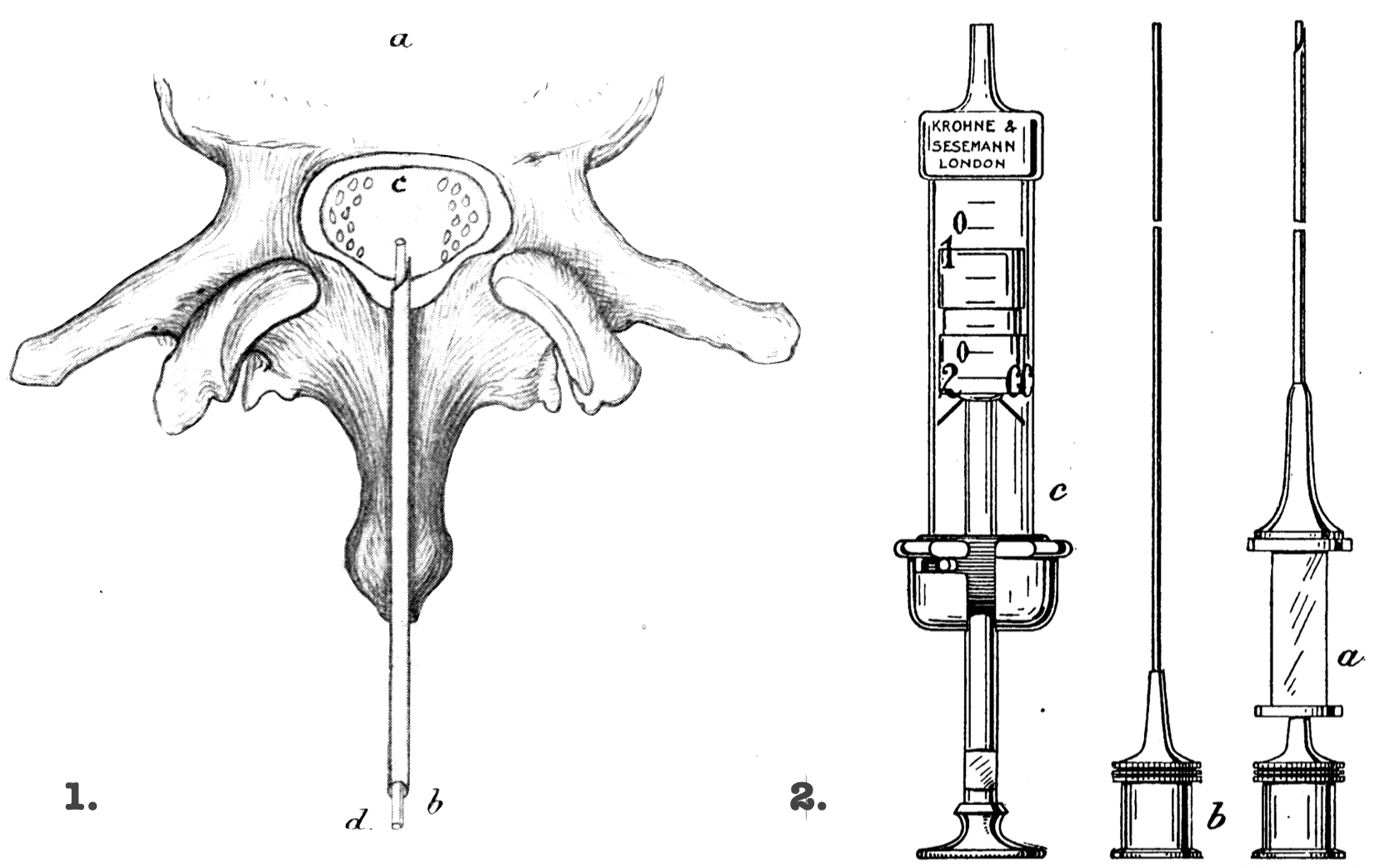
2. Barker’s spinal analgesia equipment (a) hollow puncture needle (b) blunt inner cannula (c) 2 mL Record syringe Barker 1907
Barker advised rotating the needle on its axis once or twice when only a few drops of CSF appeared, without pushing further in. He believed this would move the dural flap aside and allow CSF pressure to help bring the whole opening into the canal. The projecting central cannula was an additional safeguard, designed to push the flap aside and deliver the drug beyond the point of the needle. Barker reported that after these precautions, injection failures fell from 6% in his first 50 cases to under 0.5% in later cases.
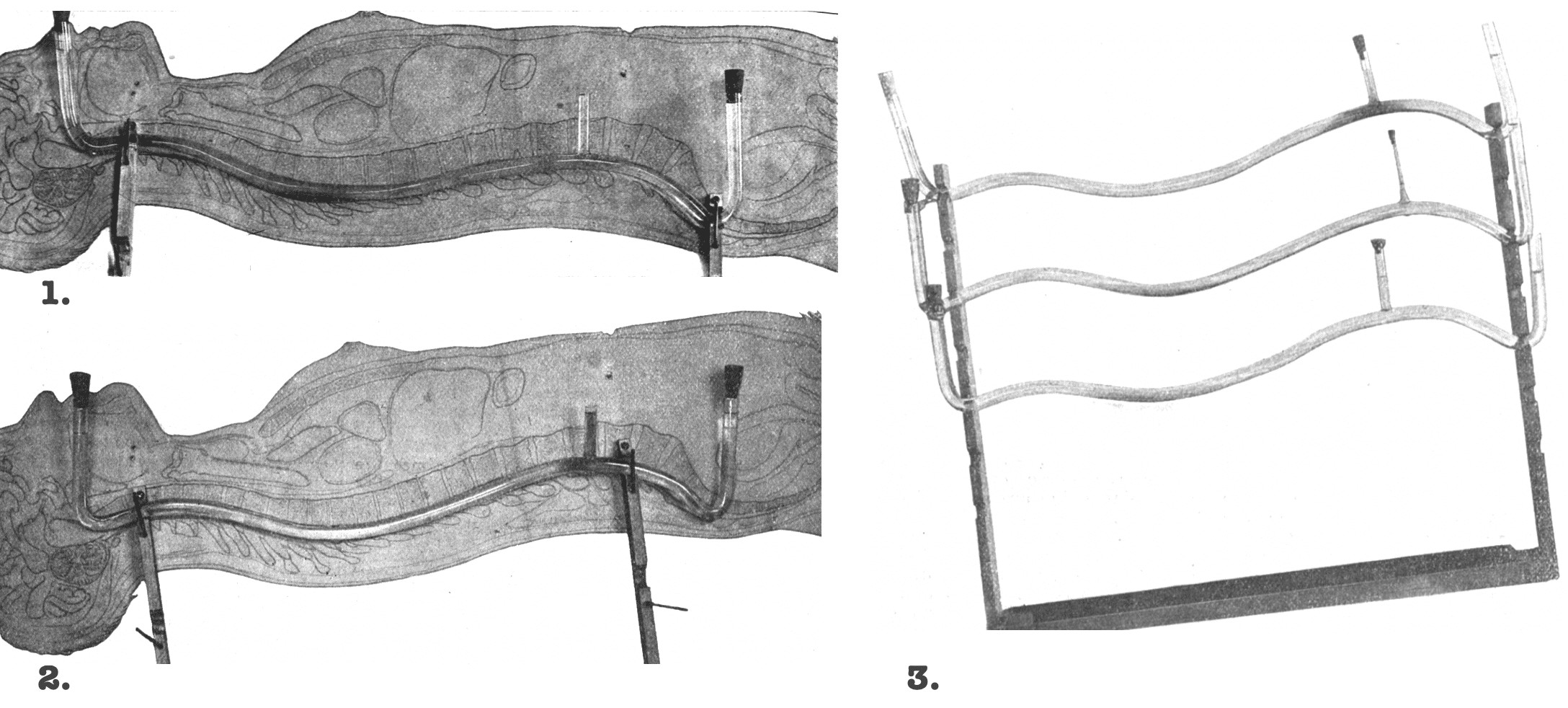
Barker’s “glass spine” and gravity control
Barker’s most important physiological contribution was his analysis of how spinal anaesthetic solutions spread within the subarachnoid space. In 1907 he tried to explain why apparently correct spinal injections could produce variable block height, duration, and distribution.
To model this, Barker constructed curved glass tubes shaped as closely as possible to the curves of the spinal canal, based on Braune’s frozen section of an adult lying supine. The tubes were filled with saline of similar specific gravity to CSF and injected with coloured analgesic solutions at different inclinations. Barker demonstrated that solution density, spinal curvature, patient position, and gravity were central to the spread of spinal analgesia.
He found that uniform results could not be expected unless the specific gravity of the injected solution was considered in relation to the CSF, and unless the patient’s posture during and after puncture was deliberately chosen.
Barker used a hyperbaric solution of 5% stovaine in 5% glucose in normal saline producing analgesia for about 50–70 minutes. For abdominal surgery, Barker injected the patient in the lateral position, using pelvic elevation with a folded blanket to direct the heavier solution toward the thoracic region of the vertebral canal. He found the highest analgesias were obtained with the patient lying quietly on the side before and after injection allowing the CSF to remain at rest.
Local analgesia infiltration
Before his spinal analgesia work, Barker was one of the earliest British surgeons to adopt and refine local infiltration analgesia. In 1899 he reported on local infiltration analgesia without the use of chloroform or ether in selected cases. He stressed that the method was not simply “haphazard” injection into the operative field, but a technique requiring practice, anatomical understanding, and careful attention to the sensory nerves supplying the region.
…it must soon become abundantly evident that the procedure does not consist in the mere injection of a certain amount of one or other drug at haphazard into the field of operation. Many factors require to be taken into very careful consideration
Barker 1899
Barker moved away from using cocaine because of toxicity and favoured β-eucaine in normal saline. In 1900 he published further experience of operations under local analgesia reporting no toxic effects even with large volumes of 1:1000 β-eucaine in normal saline. He did recognise limitations in children, timid adults, and procedures where complete infiltration was impractical.
In 1903 Barker publsihed his improvements in the methods of local analgesia incorporating Braun’s vasoconstrictor principle by adding adrenaline to prolong and intensify local analgesia. His preferred solution was β-eucaine 0.2 g, sodium chloride 0.8 g, distilled water 100 mL, and adrenaline chloride 1:100,000. He noted that adrenaline alone had no analgesic effect, but when combined with β-eucaine it produced better and longer analgesia.
Aseptic surgical technique
Barker was an important British pioneer of aseptic surgical technique. He moved from carbolic antisepsis toward the newer German-influenced aseptic system of heat sterilisation, theatre discipline, and prevention of contamination. Barker was one of the first surgeons in England to adopt the heat-sterilisation methods associated with Ernst von Bergmann and Carl Schimmelbusch. His recommendations on gowns, gauze face coverings, gloves, and “no-touch” technique helped shape British surgical practice.
His 1906 lecture on the hands of surgeons and assistants in operations reviewed the possible routes by which infection could enter a wound. Including from the patient’s own body, surrounding air, contaminated instruments, ligatures, swabs, dressings, clothing, and the hands of the surgeon or assistants. He argued that infection from instruments, dressings, and swabs could largely be prevented by boiling or steam sterilisation, but that the patient’s skin and the surgical hand remained persistent sources of risk.
…we are obliged to admit that the hand is almost impossible to sterilise and to keep sterile.
Barker promoted a practical ritual of preoperative skin cleansing, sterile draping, limited personnel, and minimal hand contact with raw tissue. He favoured hot baths, scrubbing, carbolic wraps, final spirit cleansing, and covering the patient with a sterile sheet with a small operative aperture. In the wound itself, he urged the use of sterile gauze and instruments rather than fingers, and that extensive operations could be performed without fresh-cut surfaces being touched by anything other than sterile gauze or steel instruments.
Major Publications
- Barker AE. A Case of Gastro-Enterostomy for Cancer of the Pylorus and Stomach: Good Recovery, a New Method of Suture. Br Med J. 1886 Feb 13;1(1311):292-4.
- Barker AEJ. A short manual of surgical operations. 1887
- Barker AEJ. Hunterian lectures on intra-cranial inflammations starting in the temporal bone : their complications and treatment. 1889
- Barker AE. Surgical affections of the stomach, and their treatment. 1898
- Barker AE. A Study of Fifty Consecutive Cases of Operation for the Radical Cure of Non-strangulated Herniæ. Med Chir Trans. 1890;73:273-96.
- Barker AE. Intussusception of the Sigmoid Flexure of the Colon Completely Removed through the Anus. Br Med J. 1892 Dec 3;2(1666):1226.
- Barker AE. A Note on the Technique of Removal of the Vermiform Appendix. Br Med J. 1895 Apr 20;1(1790):863.
- Barker AE. Notes on the Permanent Subcutaneous Method of Wiring the Patella for Fresh Transverse Fracture. Br Med J. 1896 Apr 18;1(1842):963-6.
- Barker AE. A New Suture for the Intestine, Mesentery, Etc. Br Med J. 1898 Jul 16;2(1959):148-9.
- Barker AEJ. Clinical lecture and demonstration on local infiltration analgesia. Lancet. 1899; 153(3936): 282-285
- Barker AEJ. A note on some further experience of operations under local analgesia produced by eucaine β. Lancet. 1900; 155(3986): 156–157.
- Barker AEJ. Clinical remarks on some improvements in the methods of local analgesia. Lancet. 1903; 162(4169): 203–206.
- Barker AE. Notes on Local Analgesia. Br Med J. 1904 Dec 24;2(2295):1682-5.
- Barker AE. Clinical lecture on the hands of surgeons and assistants in operations. Lancet. 1906; 168(4328) :345–348.
- Barker AE. A report on clinical experiences with spinal analgesia in 100 cases and some reflections on the procedure. Br Med J. 1907 Mar 23;1(2412):665-74.
- Barker AE. A Second Report on clinical experiences with spinal analgesia: with a second series of one hundred cases. Br Med J. 1908 Feb 1;1(2457):244-9.
- Barker AE. A Third Report on clinical experiences with spinal analgesia: with a third series of one hundred cases. Br Med J. 1908 Aug 22;2(2486):453-5.
- Barker AE. A Fourth Report on experiences with spinal analgesia in reference to 2,354 cases. Br Med J. 1912 Mar 16;1(2672):597-602.
- Barker AEJ. Progress in intestinal surgery. Br Med J 1909;2:263
- Barker AEJ. Leukoplakia. Practitioner. 1914; 93: 176.
References
Biography
- Arthur Edward James Barker. Lancet 1916; 187(4834): 883
- Arthur Edward James Barker, F.R.C.S. (England and Ireland), Professor of Surgery, University College Hospital Medical School, Consulting Surgeon to Queen Alexandra’s Military Hospital, Millbank, Surgeon to University College Hospital, Colonel, Army Medical Service. BJS 1916; 4(13): 11-13
- Barker, Arthur Edward James (1850 – 1916) Plarr’s Lives of the Fellows
Eponymous terms
- Lee JA. Arthur Edward James Barker 1850-1916. British pioneer of regional analgesia. Anaesthesia. 1979 Oct;34(9):885-91.
- Harms R, Cadogan M. History of Spinal Needles. LITFL
Eponym
the person behind the name
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |