
![]()
History of Spinal Needles
Spinal needles are fine hollow needles used to enter the subarachnoid space, confirm position by free flow of cerebrospinal fluid, and inject local anaesthetic directly into CSF. They are used for spinal anaesthesia, diagnostic lumbar puncture, intrathecal drug delivery, and related neuraxial techniques.
The history of spinal needle development involves a series of compromises. How to make a needle sharp enough to reach the CSF reliably, but small and atraumatic enough to minimise CSF leak, post-dural puncture headache (PDPH), failed block, and neurological injury.
Spinal needles evolved from the hollow cannula, syringe, injectable local anaesthetic, and anatomical access to the spinal canal. Unlike epidural needles, which are designed to identify the epidural space without deliberately puncturing the dura, spinal needles intentionally cross the dura and arachnoid to enter the subarachnoid space. Free CSF flow became the defining endpoint of spinal anaesthesia.
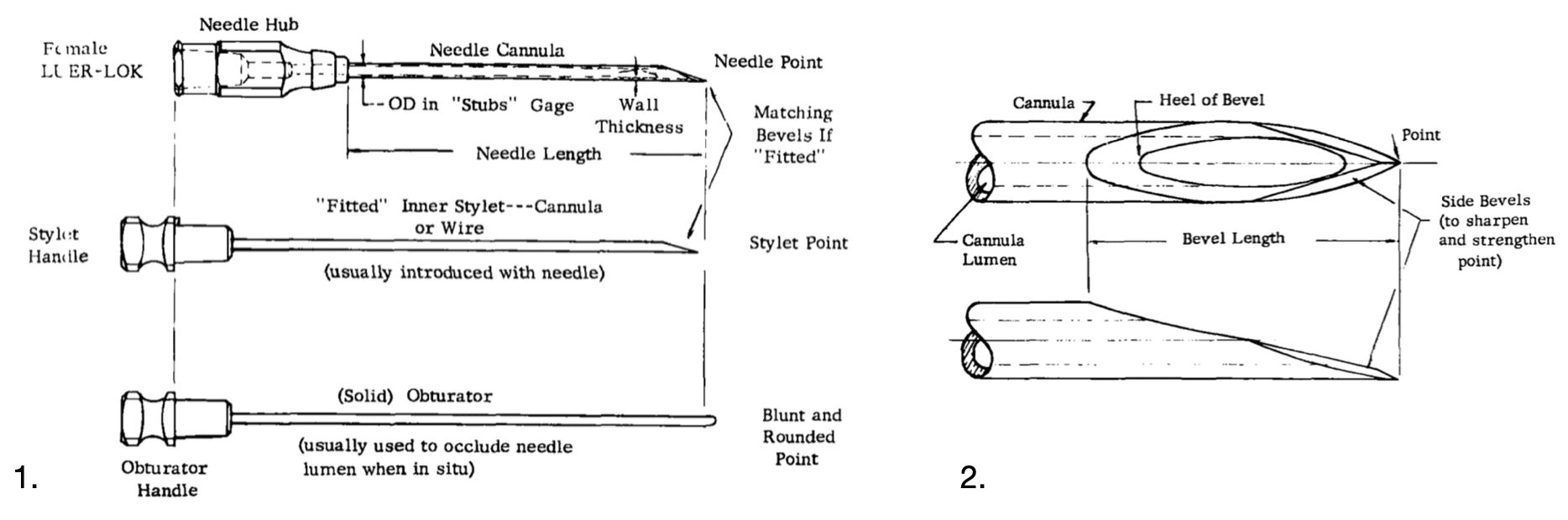
Early spinal needles were modified hypodermic or lumbar puncture needles which were hollow, bevelled, reusable, and large by modern standards. Over the last 150 years, design moved from large cutting-bevel needles toward smaller gauge needles, matching stylets, introducer systems, rounded or blunted points, lateral orifices, and finally pencil-point atraumatic designs. Modern 22–27G pencil-point needles with lateral orifices reflect repeated attempts to enter CSF reliably while leaving the smallest, least persistent dural defect.
The principal eponymous designs include the Quincke, Barker, Quincke–Babcock, Labat, Greene, Pitkin, Whitacre, and Sprotte needles. Transitional figures such as Hoyt, Sise, Haraldson, Lemmon, and Tuohy connect this single-shot spinal needle story with fine-gauge lumbar puncture, continuous spinal anaesthesia, and later epidural catheter practice.
Design variables in spinal needles
Gauge / diameter: Smaller needles reduce dural trauma and PDPH risk, but are harder to direct and produce slower CSF flow.
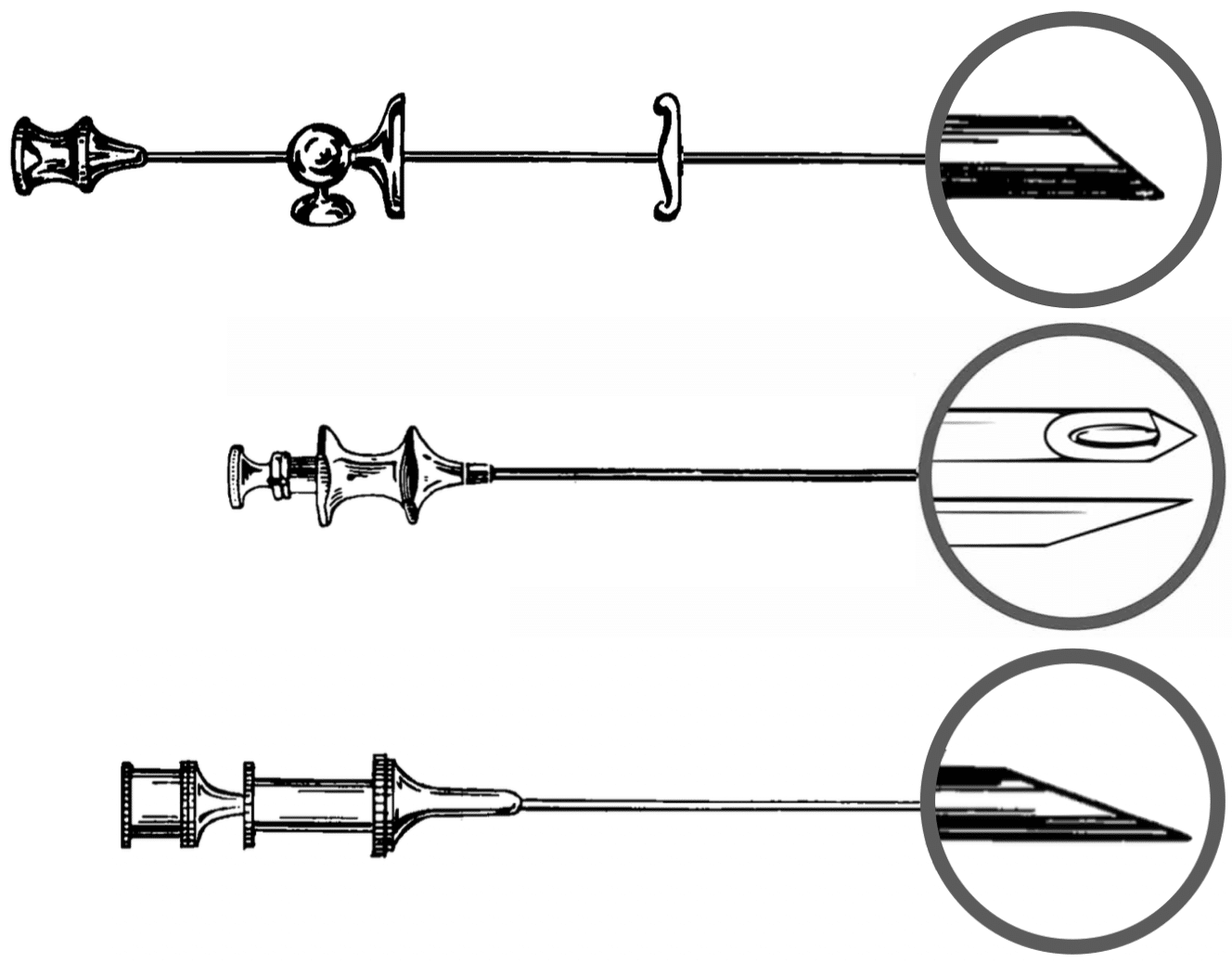
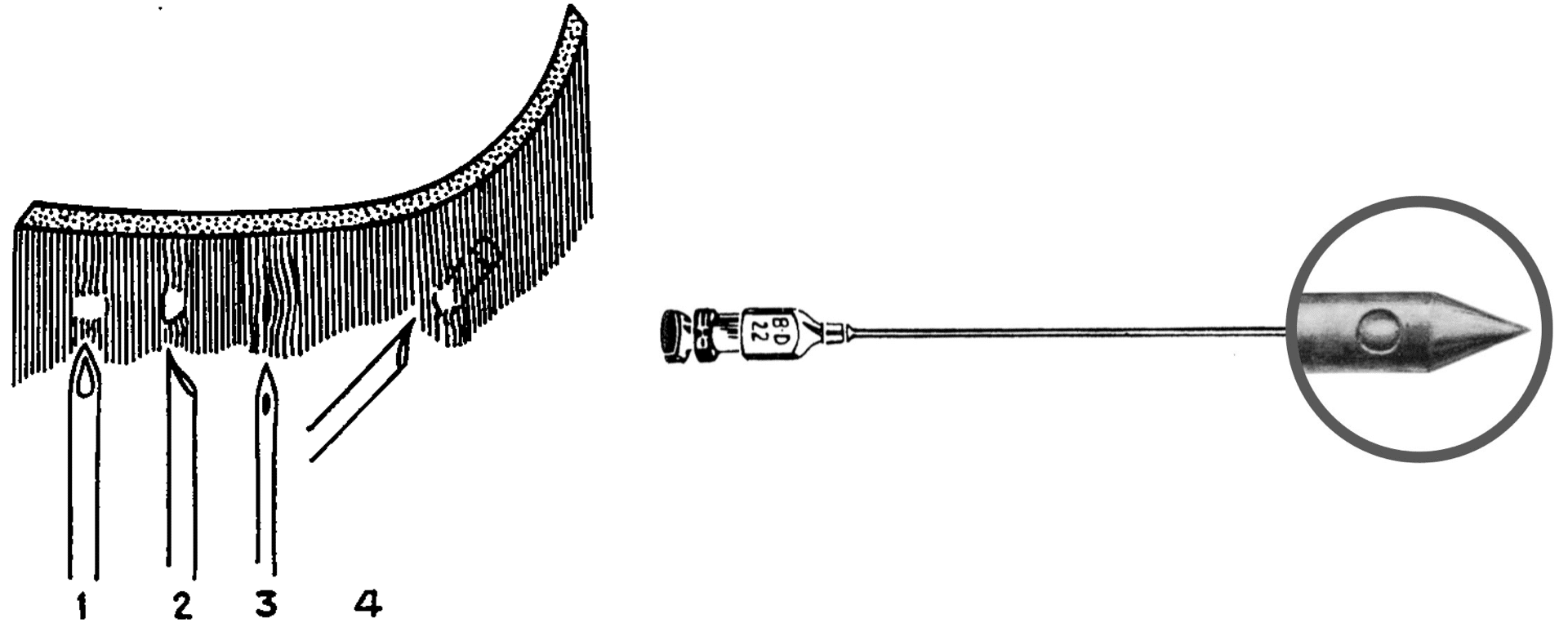
Tip design: Cutting bevels enter easily but cut dural fibres. Rounded, blunted, stylet-tip, and pencil-point designs aim to separate rather than incise fibres.
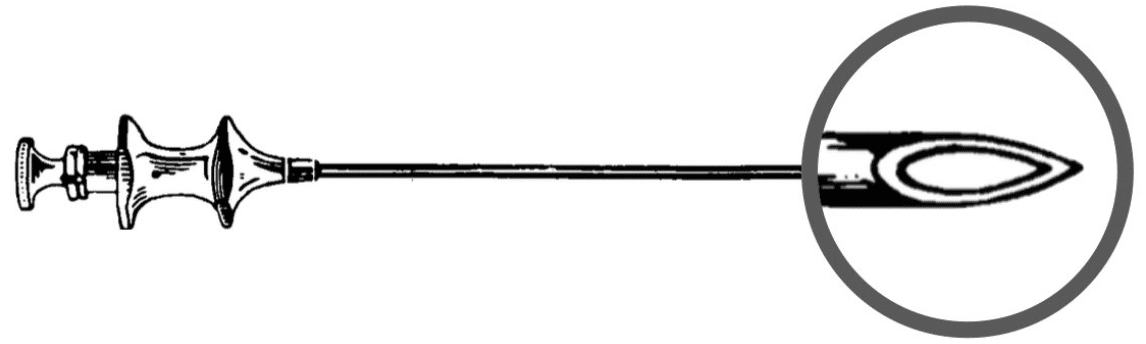
Orifice position: Terminal openings risk Barker’s “orifice straddling the dura” problem. Pencil-point needles move the orifice to the side, requiring the lateral opening to be fully intrathecal before injection.
Stylets and introducers: Matching stylets reduce coring and obstruction. Introducers allow fine needles to pass through skin and ligament without bending.
Materials: Early gold, platinum, nickel, and plated steel needles were soft, brittle, or corrosion-prone. Rustproof steel and disposable manufacture made finer, safer needles practical.
Spinal anaesthesia and spinal needle history timeline
Foundations and hardware
1764 – Cotugno and early CSF anatomy. Domenico Felice Antonio Cotugno (1736–1822), Italian physician, described fluid around the brain and spinal column and early anatomical context for later CSF access. [Cotugno 1764]
1825 – Magendie and CSF circulation. François Magendie (1783–1855), French physiologist, described the “liquide céphalo-rachidien ou cérébro-spinal” (cerebrospinal fluid) and its circulation around the brain and spinal cord. [Magendie 1825]
1845 – Rynd and the hollow cannula. Francis Rynd (1801–1861), Irish surgeon, used a hollow cannula and gravity-flow device to introduce medication subcutaneously for neuralgia. This was an early functional hypodermic concept and a precursor to injection-based regional anaesthesia. [Rynd 1845]
1853–1855 – Pravaz, Wood, and the syringe-needle system. Charles Gabriel Pravaz (1791–1853), French surgeon, developed a screw-driven syringe and trocar-cannula system. Alexander Wood (1817–1884), Scottish physician, popularised syringe-and-needle therapeutic injection. [Pravaz 1853; Wood 1855]
1884 – Koller and injectable local anaesthesia. Carl Koller (1857–1944), Austrian ophthalmologist, introduced cocaine as a practical local anaesthetic. Hollow needles could now deliver analgesia, not just remove or inject fluid. [Koller 1884]
Early spinal concept and lumbar puncture
1885 – Corning and the spinal anaesthesia concept. James Leonard Corning (1855–1923), American neurologist, introduced the term “spinal anaesthesia” after neuraxial cocaine experiments using a short-bevel gold/platina needle with introducer and depth stop. Later analysis suggests his injection was probably epidural rather than truly intrathecal. [Corning 1885]
1891 – Wynter and CSF drainage. Walter Essex Wynter (1860–1945) English physician, described lumbar thecal puncture and drainage for raised CSF pressure in tuberculous meningitis. His approach was surgical, but remains important in the priority debate over the first lumbar puncture. [Wynter 1891]
1891 – Quincke and lumbar puncture. Heinrich Irenäus Quincke (1842–1922), German physician, standardised lumbar puncture using a sharp bevelled hollow needle for CSF pressure relief and sampling. The Quincke cutting-bevel needle became the archetype from which early spinal needles evolved. [Quincke 1891]
1899 – Bier and the PDPH problem. August Karl Gustav Bier (1861–1949), German surgeon, performed the first widely accepted surgical spinal anaesthetics using cocaine. His early cases and self-experimentation demonstrated both the promise of spinal anaesthesia and the severe post-dural puncture headache that would drive spinal needle design for the next century. [Bier 1899]
1900 – Tuffier and the CSF endpoint. Théodore Tuffier (1857–1929), French surgeon, emphasised that cocaine should not be injected until CSF was identified. This principle remains the defining practical distinction between spinal and epidural anaesthesia: spinal anaesthesia has a visible CSF endpoint; epidural anaesthesia relies on indirect localisation signs. [Tuffier 1900]
1900 – Kreis and obstetric spinal anaesthesia. Oskar Kreis (1872–1958), Swiss obstetrician–gynaecologist, published early spinal cocaine analgesia for childbirth. Obstetric spinal practice later became a major driver for smaller, less traumatic needles because young postpartum patients were especially vulnerable to PDPH. [Kreis 1900]
Cutting bevel era: reliability versus dural trauma
1900 – Bainbridge and controlled spinal injection hardware. William Seaman Bainbridge (1870–1947), American surgeon and gynaecologist, described paediatric and adult spinal analgesia using a flexible metal needle attached to a metal syringe, with a short cutting bevel and matching stylet. This marked a move from improvised puncture equipment toward purpose-built intrathecal injection hardware.[Bainbridge 1900]
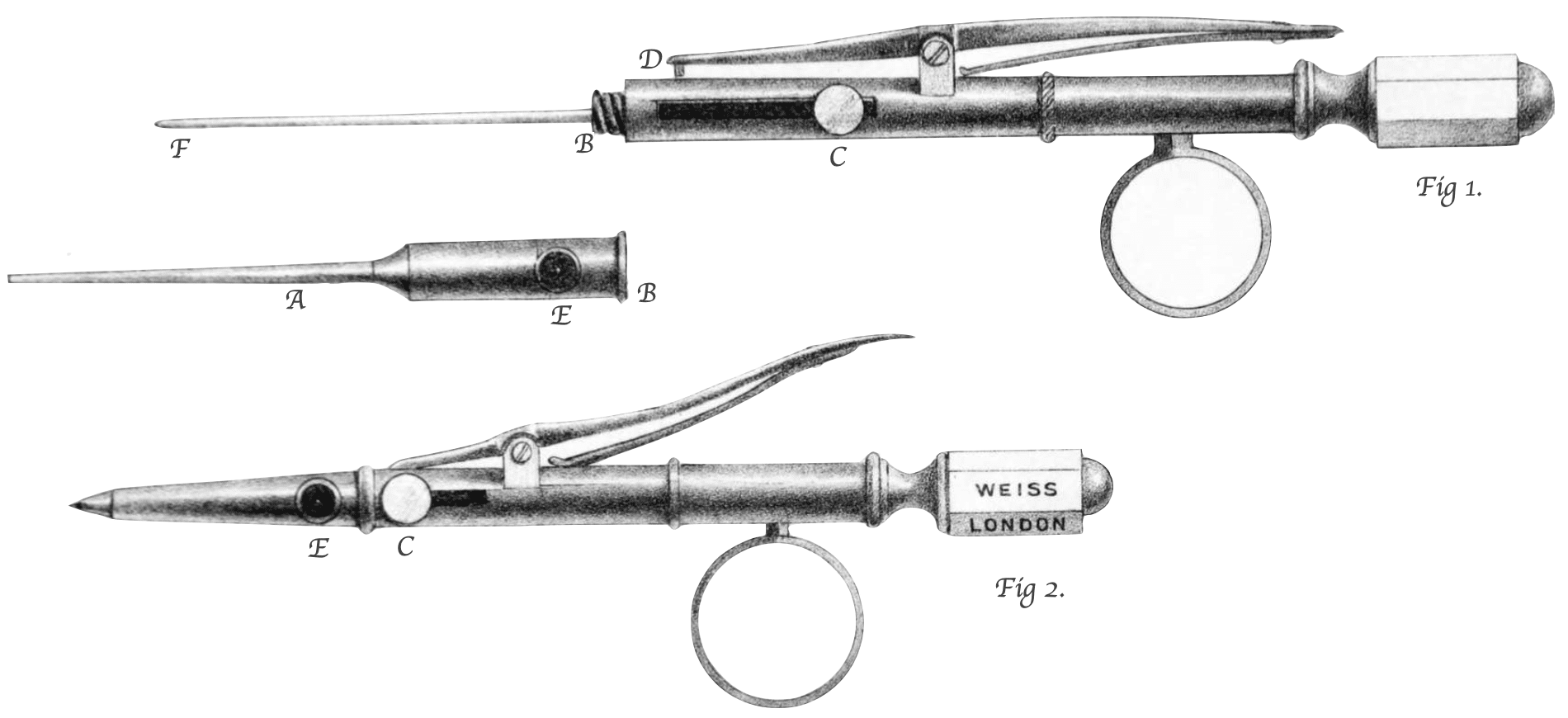
1907 – Barker and the “orifice straddling the dura” problem. Arthur Edward James Barker (1850–1916), Irish-born British surgeon, recognised that CSF could appear at the hub even when the terminal needle opening was only partly intrathecal. His projecting blunt inner cannula delivered anaesthetic beyond the needle tip into the dural sac. [Barker 1907]
1914 – Babcock and the Quincke–Babcock needle. William Wayne Babcock (1872–1963), American surgeon, helped standardise early American spinal anaesthesia technique. The later-named Quincke–Babcock needle was a smaller styleted 20G cutting-bevel spinal needle with a medium bevel and matching stylet. [Babcock 1914]
Smaller needles, introducers, and better materials
1921 – Labat and the short-bevel nickel spinal needle. Louis Gaston Labat (1876–1934), French-trained regional anaesthesia pioneer, described a purpose-built nickel spinal puncture needle with medium gauge, medium length, short bevel, and matching stylet. His sterilizable Labat regional anaesthesia outfit placed the spinal needle within a broader system of standardised regional anaesthesia equipment. [Labat 1921; Labat 1922]
1923 – Herbert Greene and the round-pointed needle. Herbert Merton Greene (1878-1962), American physician, linked post-lumbar puncture headache to dural trauma and CSF leakage. His microphotographs of punctured dura supported a small, smooth, round-pointed needle designed to pass between dural fibres rather than cut them. [Greene 1923; Greene 1926]
1927 – Pitkin and the trapdoor theory. George Philo Pitkin (1885-1943), American surgeon, promoted “controllable spinal anaesthesia” and a short blunted-bevel spinal needle. His “trapdoor” theory of dural closure was later questioned, but raised the important concept that needle-tip geometry affects CSF leakage and PDPH. [Pitkin 1927]
1928 – Sise and fine-gauge needle control. Lincoln Fleetford Sise (1874–1942), American anaesthetist at the Lahey Clinic, described a flanged introducer cannula to facilitate fine-gauge lumbar puncture needles. Fine needles reduced post-puncture headache, but Sise’s device made them easier to control through skin and ligament. [Sise 1928]
1920s – The shift from size to shape. By the end of the 1920s, spinal needle design moved beyond the concept that “smaller is safer.” Smaller diameter remained important, but designers increasingly recognised that tip shape, bevel length, orifice position, material, introducer use, and dural fibre disruption all contributed to PDPH and block reliability.

Continuous spinal and directional needles
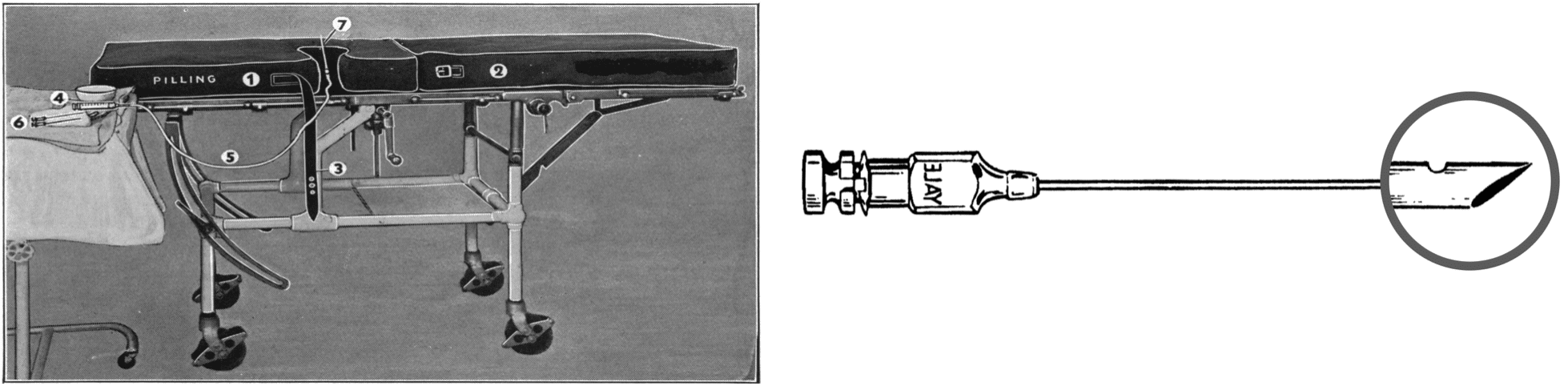
1940 – Lemmon and continuous spinal anaesthesia. William Thomas Lemmon (1896–1974), American surgeon, developed continuous spinal anaesthesia using a malleable needle left in the subarachnoid space and a specialised mattress system. Cumbersome in practice, it was important as a bridge toward titratable neuraxial techniques. [Lemmon 1940]
1944 – Rovenstine and directional spinal needles. Emery Andrew Rovenstine (1895–1960), American anaesthesiologist, with Sarnoff, described a directional spinal anaesthesia needle. Part of the spinal-to-epidural transition where needle direction and catheter passage became important design problems. [Sarnoff, Rovenstine 1944]
1945 – Tuohy and continuous spinal catheter technique. Edward Boyce Tuohy (1908–1959), American anaesthesiologist, published catheter-through-needle continuous spinal anaesthesia. His name is now chiefly linked to epidural needles, but his early is important in continuous spinal. [Tuohy 1945]
Continuous spinal as a transitional idea. Continuous spinal anaesthesia never displaced single-shot spinal anaesthesia in routine practice. Technical complexity, infection concern, PDPH risk, catheter problems, and later concern about neurological complications limited its adoption. However, the technique helped focus attention on needle direction, catheter passage, and titratable neuraxial blockade.
Fine-gauge obstetric and pencil-point era
1950 – Barnett Greene and fine-gauge obstetric spinal needles. Barnett Alan Greene (1907-1999), American anaesthesiologist, published on fine-gauge 24G and 26G lumbar puncture needles for obstetric spinal analgesia. His work reduced post-spinal headache after vaginal delivery and should be distinguished from Herbert Merton Greene’s earlier round-pointed needle work. [Greene BA 1950]
1951 – Haraldson and the early non-cutting lateral-orifice needle. Sixten Haraldson, Swedish anaesthetist, described an early tapered non-cutting spinal needle with a lateral orifice. His design sits between early rounded/blunted needles and the Whitacre needle. [Haraldson 1951]
1951 – Whitacre, Hart and the pencil-point needle. Rolland John Whitacre (1909–1956), and James R. Hart, American anaesthesiologists, introduced the Whitacre pencil-point spinal needle. Its solid conical tip and lateral orifice were designed to separate rather than cut dural fibres, reducing PDPH compared with cutting needles. [Hart, Whitacre 1951]
1979 – Sprotte and the long lateral-orifice pencil-point needle. Günter Sprotte (1945- ), German anaesthetist, with Horst Pajunk, developed the Sprotte pencil-point spinal needle. Its long lateral orifice improved CSF flow but required the entire opening to lie intrathecally before injection. [Pajunk, Sprotte 1979, Sprotte 1987]
Late twentieth-century and modern designs
1970s–1980s – Atraumatic spinal needles and obstetric resurgence. Earlier obstetric spinal practice had been limited by hypotension and PDPH. Smaller, non-cutting needles reduced severe headache and encouraged renewed interest in single-shot spinal and combined spinal–epidural techniques. The combination of improved needle design, better understanding of maternal physiology, and more active management of hypotension allowed spinal anaesthesia to return as a practical technique.
1993 – Atraucan needle. The Atraucan needle was introduced as a double-bevel cutting-tip design intended to balance ease of dural puncture with reduced tissue trauma. It was not a pure pencil-point needle, but an attempt to preserve the handling advantages of cutting needles while reducing dural injury.
1990s–2000s – Double-hole, ballpen, and tip-hole designs. Later spinal needle designs explored double side holes, modified pencil-points, ballpen-style tips, and tip-hole variants. Designs continue to address the same fundamental problems of how to confirm intrathecal position, minimise dural trauma, and manage failed block, CSF leakage, and PDPH.
The modern spinal needle is not a single solved design, but the result of a century of development refining tactile feedback, CSF flow, injection reliability, manufacturing practicality, and the smallest possible dural injury.
References
Historical references
- Cotugno DFA. De ischiade nervosa commentaries, Naples Fratres Simonios, 1764
- Magendie F. Mémoire sur un liquide qui se trouve dans le crâne et la colonne vertébrale de l’homme et des animaux mammifères. Journal de Physiologie Expérimentale et Pathologique. 1825; 5: 27-37
- Magendie F. Recherches physiologiques et cliniques sur le liquide céphalo-rachidien ou cérébro-spinal. 1842
- Jayne Z. Method of treating reducible hernia. US Patent 2032. April 2, 1841
- Rynd F. Neuralgia – introduction of fluid to the nerve. Dublin Med Press 1845; 13: 167–168
- Pravaz. Sur un nouveau moyen d’opérer la coagulation du sang dans les artères, applicable à la guérison des anévrismes. Comptes rendus hebdomadaires des séances de l’Académie des sciences 1853; 36(2): 88-90
- Wood A. New method of treating neuralgia by the direct application of opiates to the painful points. Edinburgh Medical and Surgical Journal 1855; 82: 265-281
- Koller C. Vorläufige Mittheilung über locale Anästhesirung am Auge. Bericht über die 16. Versammlung der ophthalmologisrhen Gesellschaft. Heidelberg. Klinische Monatsblätter für Augenheilkunde 1884; 22: 60-63
- Corning JL. Spinal anaesthesia and local medication of the cord. New York Medical Journal 1885; 42: 483-485
- Quincke HI. Die lumbalpunction des hydrocephalus. Berliner Klinische Wochenschrift 1891; 28: 929-933 and 965-968
- Bier A. Versuche über Cocainisirung des Rückenmarkes. Deutsche Zeitschrift für Chirurgie 1899; 51: 361. [Translated: Experiments Regarding the Cocainization of the Spinal Cord. Survey of Anesthesiology 1962; 6: 352–358]
- Wynter WE. Four cases of tubercular meningitis in which paracentesis was performed for the relief of fluid pressure. Lancet 1891 May 02; 137(3531): 981-982
- Tuffier T. Anesthésie medullaire chirurgicale par injection sous-arachnoidienne lombaire de cocaine; technique et results. Semaine médicale 1900; 20: 167–169
- Bainbridge WS. Analgesia in children by spinal injection with a report of a new method of sterilization of the injection fluid. Medical Record. 1900; 58: 937-940
- Kreis O. Über Medullarnarkose bei Gebärenden. Zentralblatt für Gynäkologie 1900; 24(28): 724–729.
- Barker AE. A report on clinical experiences with spinal analgesia in 100 cases and some reflections on the procedure. British Medical Journal 1907; 1: 665–74.
- Babcock WW. The technic of spinal anesthesia. New York Medical Journal 1914; 100(15): 697–702.
- Labat GL. Latest achievements of the art of local, regional and spinal anesthesia. Ann Surg. 1921 Dec;74(6):673-83
- Greene HM. A technic to reduce the incidence of headache following lumbar puncture in ambulatory patients with a plea for more frequent examination of cerebrospinal fluids. Northwest Medicine 1923; 22(7): 240–5
- Greene HM. Lumbar puncture and the prevention of postpuncture headache. Journal of the American Medical Association 1926; 86(6): 391-392
- Greene BA. A 26 gauge lumbar puncture needle: its value in the prophylaxis of headache following spinal analgesia for vaginal delivery. Anesthesiology. 1950 Jul;11(4):464-9.
- Pitkin GP. Controllable spinal anesthesia. Journal of the Medical Society of New Jersey 1927; 24: 425–38.
- Sise LF. A device for facilitating the use of fine gauge lumbar puncture needles. Journal of the American Medical Association 1928;91;(16):1186
- Kirschner M. Spinal zone anesthesia. Surgery Gynecology and Obstetrics 1932; 55: 317–29.
- Lemmon WT. A method for continuous spinal anesthesia: A preliminary report. Ann Surg. 1940 Jan;111(1):141-4
- Sarnoff SJ, Rovenstine E. A directional spinal anesthesia needle. Anesthesiology 1944; 5(4): 413.
- Tuohy EB. Continuous Spinal Anesthesia: Its usefulness and technic involved. Anesthesiology 1944;5:142-148
- Tuohy EB. Continuous Spinal Anaesthesia: A new method utilizing a ureteral catheter. Surg clin North AM 1945;25:834-840
- Haraldson S. Headache after spinal anesthesia: experiments with a new spinal needle. Anesthesiology. 1951 May;12(3):321-7.
- Hart JR, Whitacre RJ. Pencil-point needle in prevention of postspinal headache. J Am Med Assoc. 1951 Oct 13;147(7):657-8.
- Pajunk H, Sprotte G. Stahlkanüle für die Spinal- und Leitungsanästhesie sowie für die Lumbalpunktion 1979 Patent
Eponymous term review
- Blake JB. Mr. Ferguson’s Hypodermic Syringe, Journal of the History of Medicine and Allied Sciences, 1960; XV(4): 337–34
- Schorr MR. Needles. Some points to think about. I. Anesth Analg. 1966 Jul-Aug;45(4):509-13
- Schorr MR. Needles some points to think about. II. Anesth Analg. 1966 Sep-Oct;45(5):514-9.
- Schorr MR. Needles some points to think about. III. Anesth Analg. 1966 Sep-Oct;45(5):520-6
- Marx GF. The first spinal anesthesia. Who deserves the laurels? Reg Anesth. 1994 Nov-Dec;19(6):429-30.
- Morgan P. Spinal anaesthesia in obstetrics. Can J Anaesth. 1995 Dec;42(12):1145-63.
- Currir DS, Bevacqua BK. Sprotte spinal needle: a new design. Reg Anesth. 1996 Mar-Apr;21(2):172-3.
- Frederiks JA, Koehler PJ. The first lumbar puncture. J Hist Neurosci. 1997 Aug;6(2):147-53.
- Marx GF. The first spinal anesthesia. Who deserves the laurels? Reg Anesth. 1994 Nov-Dec;19(6):429-30.
- Frölich MA, Caton D. Pioneers in epidural needle design. Anesth Analg. 2001 Jul;93(1):215-20.
- Goerig M, Freitag M, Standl Th. One hundred years of epidural anaesthesia—the men behind the technical development. International Congress Series, 2002; 1242: 203–212
- Ball C, Westhorpe R. Local anaesthesia–the early evolution of spinal needles. Anaesth Intensive Care. 2003 Dec;31(6):611
- Calthorpe N. The history of spinal needles: getting to the point. Anaesthesia. 2004 Dec; 59(12): 1231-41.
- Herbowski L. The maze of the cerebrospinal fluid discovery. Anat Res Int. 2013;2013:596027.
- Waurick K, Waurick R. Epiduralanästhesie – Geschichte und Technik der Epiduralanästhesie [History and Technique of Epidural Anaesthesia]. Anasthesiol Intensivmed Notfallmed Schmerzther. 2015 Jul;50(7-8):476-82
- Boulton T. Spinal anaesthesia during the 19th and 20th Centuries – cocaine and controversy. Anaesthesia News Digital April 2021
- Chinn GA, Gray AT, Larson MD. Overcoming Obstacles: The Legacy of Fidel Pagés, Founder of the Epidural, 100 Years After His Passing. Anesth Analg. 2024 Feb 1;138(2):475-479.
- Harms R, Cadogan M. History of Neuraxial Anaesthesia. LITFL
eponymictionary
the names behind the name

BSc MD, University of Western Australia (UWA). Medical interests in critical care, FOAMed and simulation training. Outside of medicine, I'm passionate about sport, camping and the outdoors.
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |