
![]()
Beighton Score
The Beighton Score is a simple, validated 9-point scoring system used to assess generalised joint hypermobility (GJH). It remains the most widely employed clinical and epidemiological tool for evaluating ligamentous laxity across populations and in diagnosing hypermobility-related conditions such as hypermobile Ehlers–Danlos Syndrome (hEDS).
The Beighton Score evaluates five physical manoeuvres, four of which are assessed bilaterally. A score of ≥4 in adults is generally considered diagnostic of GJH, although thresholds vary in paediatrics and by sex and ethnicity.
The Beighton Score
- Ability to touch palms flat to floor with knees straight (one point)
- Elbow extension >10° (one point for each side)
- Knee extension >10° (one point for each side)
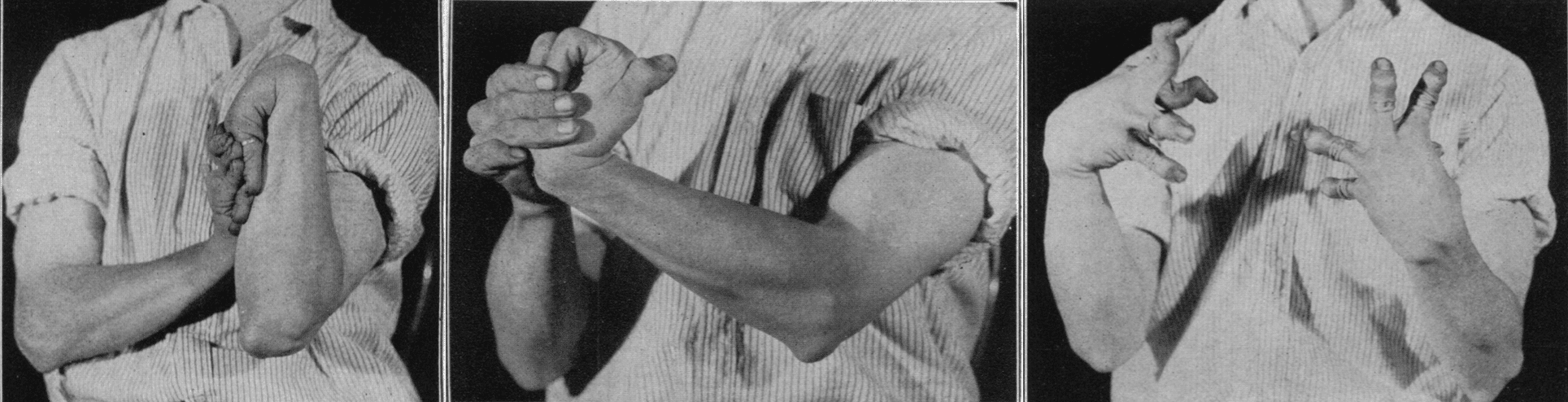
- Ability to touch thumb to forearm (one point for each side)
- Fifth finger metocarpalphalageal joint extension >90° (one point for each side)
Scores of 4 or more indicate Generalised Joint Hypermobility.
Patients may be asymptomatic, or have associated joint pain (exacerbated by exercise), dislocations and fatigue. Chronic pain often leads to muscle weakness.
Other associations include dizziness and syncope and gastrointestinal problems such as chronic abdominal pain and constipation.
While praised for its simplicity and utility, the Beighton Score’s limitations have drawn increasing attention in recent years. The joints assessed are predominantly in the upper limbs, and the score may fail to identify GJH when hypermobility is present at excluded sites, such as the shoulders, hips, or temporomandibular joints. Furthermore, the score is sensitive to age, sex, ethnicity, and even dominant-hand bias, with joint laxity tending to diminish with age and being more pronounced in females and certain ethnic groups.
Though initially designed for population surveys, the Beighton Score has been adopted into major diagnostic criteria, including the International Classification of the Ehlers–Danlos Syndromes (2017). However, critics argue that it should not be the sole tool to confirm or exclude GJH, urging clinicians to incorporate broader phenotypic assessments and historical data.
Originally developed in the early 1970s by Greta and Peter Beighton, the score is now routinely used in paediatric, orthopaedic, rheumatological, and genetic clinics.
The eponym honours the collaborative contributions of Professor Peter Beighton and Greta Beighton (née Winch), whose clinical and anthropological fieldwork in South Africa in the early 1970s refined and popularised the score. Although Greta Beighton was deliberately omitted from authorship of the original publication for fear of nepotism, her pivotal insight that joints are functionally paired but not necessarily symmetrical led directly to the modern 9-point system.
History of the Beighton Score
1927 – Early clinical observation of hereditary joint hypermobility. Orthopaedic surgeon John Albert Key (1890–1955) published a case series of a “double-jointed” family in JAMA, describing sex-linked hereditary joint hypermobility involving four sons but no daughters. The father exhibited similar features, and the report includes hyperextension of knees, elbows, and fingers.
1964 – Cedric Carter and John Wilkinson proposed a standardised method and five-point score for the clinical assessment of joint hypermobility. This formed the conceptual basis of later Beighton adaptations
- Passive apposition of the thumb to the flexor aspect of the forearm
- Passive hyperextension of the fingers so that they lie parallel with the extensor aspect of the forearm
- Ability to hyperextend the elbow more than 10 degrees
- Ability to hyperextend the knee more than 10 degrees
- Excess range of passive dorsiflexion of the ankle and eversion of the foot

1967 – Kirk, Ansell, and Bywaters define the “Hypermobility Syndrome” as a distinct clinical entity associated with musculoskeletal symptoms in hypermobile individuals.
1967-1968 – Peter Beighton undertook a clinical study of over 100 families with Ehlers-Danlos Syndrome (EDS) in Southern England, applying Carter and Wilkinson’s 5-point system. He was assisted by Greta Winch (later Greta Beighton).
1969 – Beighton and Frank T. Horan (1933-2015) explored the orthopaedic manifestations of EDS; the utility of joint mobility scores; and demonstrated the dominant inheritance patterns of generalised joint hypermobility
1970 – Peter and Greta Beighton travelled to South Africa to undertake an epidemiological investigation of bone and joint disorders, based at the University of the Witwatersrand. An initial recognisance was undertaken in a semi-nomadic Bushmen community in the Kalahari Desert. Project plans were discussed while sitting around the camp fire. Greta had a flash of insight and suggested that although the limbs and digital joins were paired, they were not necessarily symmetrical and that a 9-point score would be appropriate.
1973 – Peter Beighton, Lionel Solomon, and Clive Soskolne publish “Articular mobility in an African population” in Ann Rheum Dis. This paper formally introduces the now-standard 9-point Beighton Score with photographic demonstration of each manoeuvre. The score was successfully used in a formal epidemiological survey of 1081 persons in a Tswana community in the Transvaal, South Africa
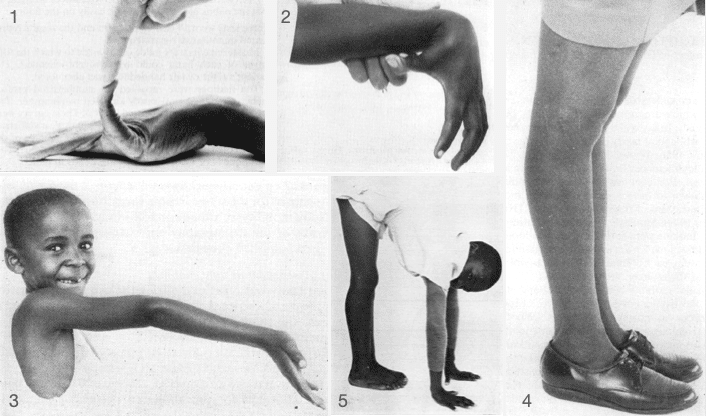
Fig. 2 Apposition of the thumb to the ventral aspect of the forearm
Fig 3. Hyperextension of the elbow joint beyond 10o
Fig 4. Hyperextension of the knee joint beyond 10o
Fig 5. Placing the palms of the hands flat on the floor while maintaining the knees in full extension
Beighton Score from Articular mobility in an African population, 1973
The method of assessing joint mobility by means of a score based upon the range of movements of certain joints has proved its value in previous investigations. Although the great majority of normal adults score values of 0, 1, or 2 on the mobility scale, individuals with inherited hypermobility syndromes achieve scores at the top end of the scale (Beighton and Horan, 1969). It is therefore reasonable to conclude that the scale is valid for the measurement of joint mobility.
The results which were obtained demonstrate that the range of movements decreases with age, falling rapidly during childhood, and more slowly throughout adult life. However, at any age, females are consistently more hypermobile than males.
Beighton et al 1973
2017 – The International Classification of the Ehlers–Danlos Syndromes incorporated the Beighton Score as a core screening tool for generalised joint hypermobility in hEDS diagnostic criteria.
2020 – Peter Beighton comments:
Following her initial suggestion in 1971 concerning the 9-point score, Greta Beighton retained her involvement in the elucidation and publication of research material in the broad field of hypermobility for almost 50 years.
During this period, she compiled ten books and more than 400 articles in medical journals. As a matter of principle, rightly or wrongly, her name was deliberately withheld from the deserved co-authorship in order to avoid any suggestion of nepotism. This article is essentially a posthumous attempt to ensure the eponymous recognition that she richly deserves.
Peter Beighton 2020, personal communication
Associated Persons
- John Albert Key (1890–1955)
- Peter Beighton (1934-2023)
- Greta Janet Beighton (1939-2017)
- Frank T. Horan (1933-2015); Orthopaedic Surgeon, UK
References
Historical references
- Key JA. Hypermobility of joints as a sex-linked hereditary characteristic. JAMA. 1927; 88: 1710-1712
- Carter C, Wilkinson J. Persistent Joint Laxity and Congenital Dislocation of the Hip. Journal of Bone and Joint Surgery, 1964; 46(1): 40-45
- Kirk, JA, Ansell, BM, Bywaters EG. The hypermobility syndrome. Musculoskeletal complaints associated with generalised joint hypermobility. 1967: 26: 419-425
- Beighton P, Horan F. Orthopaedic aspects of the Ehlers-Danlos syndrome. J Bone Joint Surg Br. 1969; 51(3): 444-453
- Beighton PH, Horan FT. Dominant inheritance in familial generalised articular hypermobility. J Bone Joint Surg Br. 1970; 52(1): 145-147.
- Horan FT, Beighton PH. Recessive inheritance of generalized joint hypermobility. Rheumatol Rehabil. 1973; 12(1): 47-49.
- Beighton P, Solomon L, Soskolne CL. Articular mobility in an African population. Ann Rheum Dis. 1973; 32(5): 413-418.
Eponymous term review
- Beighton P, de Paepe A, Danks D, Finidori G, Gedde-Dahl T, Goodman R, Hall JG, Hollister DW, Horton W, McKusick VA, Opitz JM, Pope FM, Pyeritz RE, Rimoin DL, Sillence D, Spranger JW, Thompson E, Tsipouras P, Viljoen D, Winship I, Young I. International Nosology of Heritable Disorders of Connective Tissue, Berlin, 1986. Am J Med Genet 1988; 29(3): 581-594 [OMIM 124490]
- Bird HA. Joint hypermobility in children. Rheumatology (Oxford). 2005; 44(6): 703-704.
- Lamari NM, Chueire AG, Cordeiro JA. Analysis of joint mobility patterns among preschool children. Sao Paulo Med J. 2005; 123(3): 119-123
- Malfait F et al. The 2017 international classification of the Ehlers-Danlos syndromes. Am J Med Genet C Semin Med Genet. 2017 Mar;175(1):8-26.
- Malek S, Reinhold EJ, Pearce GS. The Beighton Score as a measure of generalised joint hypermobility. Rheumatol Int. 2021 Oct;41(10):1707-1716.
- Bayomy AF, Forrester LA, Crowley SG, Popkin CA. Eponyms in Pediatric Sports Medicine: A Historical Review. Open Access J Sports Med. 2021 Jan 14;12:11-22.
eponymictionary
the names behind the name

MBBS (Hons) FCEM. Emergency Consultant at St Mary's Hospital, Imperial College Healthcare NHS Trust
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |