
![]()
Bell’s palsy
Description
Bell’s palsy: Acute idiopathic unilateral paralysis of the facial nerve.
The prototypic case is a lower motor neuron lesion of the facial nerve that presents after a viral prodrome. The patient wakes up in morning and notices in the mirror signs of facial nerve paralysis. Aetiology is most commonly vascular, inflammatory or viral. Risk factors include pregnancy, obesity, hypertension and diabetes
Signs/Symptoms
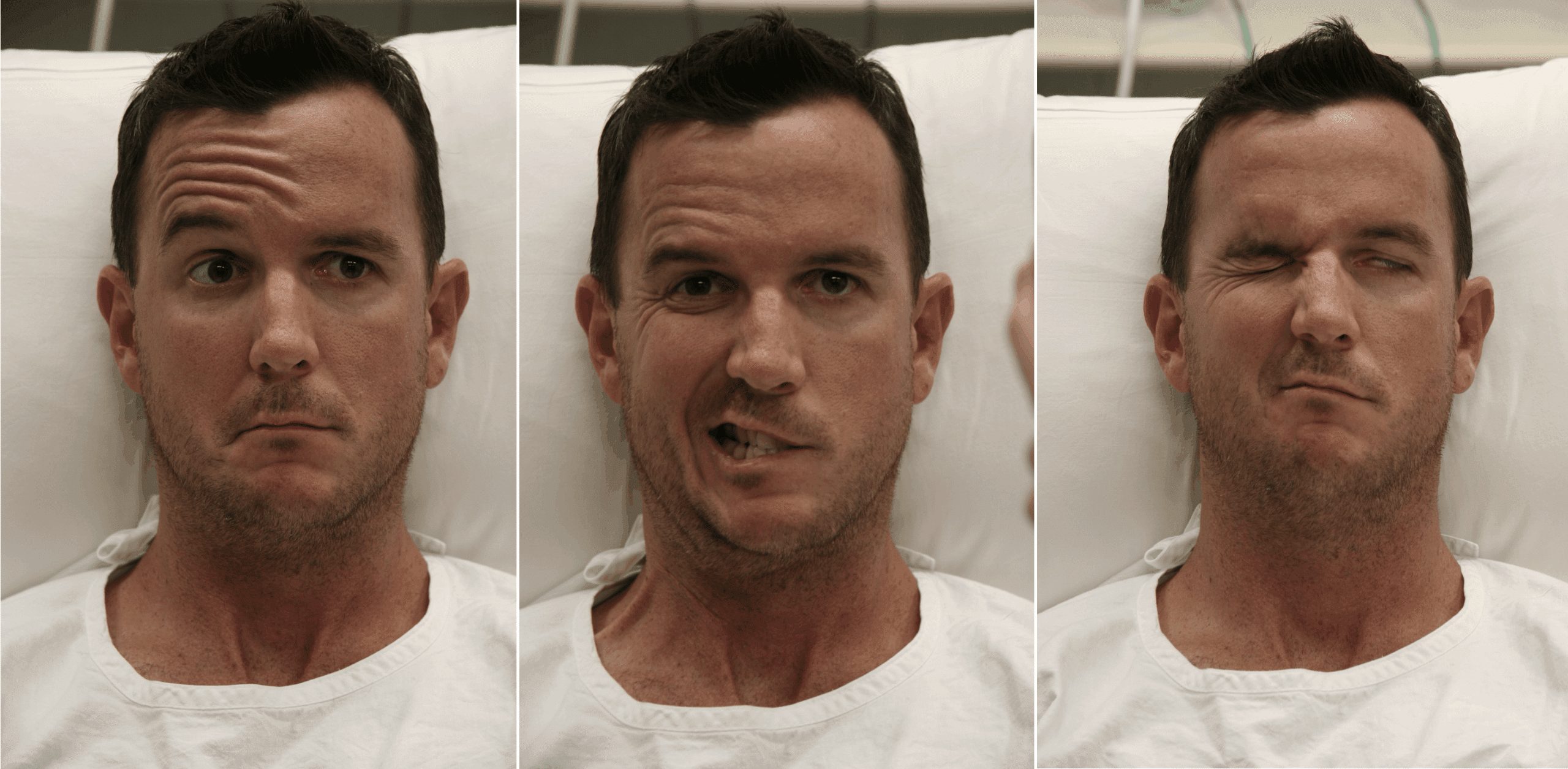
- Drooping of eyelid or an inability to completely close the eye
- Drooping of the corner of the mouth
- Unable to raise an eyebrow or wrinkle the forehead
Additional symptoms (related to facial nerve function)
- Dry eye with epiphora (excessive tearing)
- Ipsilateral loss of taste sensation
- Hyperacusis
Differential diagnosis
- Central Lesion of the facial nucleus of the brain stem, UMNL
- Ramsy Hunt syndrome (Herpes Zoster oticus), painful rash in ear
- Miller Fisher variant GBS
- Note: Can present as a polyneuritis involving trigeminal, glossopharyngeal, 2nd cervical or vagal nerve.
Course and treatment
- Usually self-limiting and resolves after 12 weeks. Up to 30% have some residual symptoms.
- Steroids help in severe cases (early complete paralysis) improves recovery time.
- The House-Brackmann grading scale can be used for assessing severity and progression.
- Most important supportive treatment is eye protection!
History of Bell’s Palsy
1020 – Avicenna (Ibn Sinh) (980-1037) – described spastic, atonic and convulsive types of facial palsy in ‘Al Qanun Fi Al-Tibb’ (The Canon of Medicine) translated into Latin in the 12th century and then into English (Gruner 1930)
1797 – Nicolaus Anton Friedreich (1761-1836) in ‘De paralysis musculorum faciei rheumatica.’ provides a detailed description of idiopathic peripheral facial nerve paralysis demonstrating careful clinical observations; deductive reasoning about the nervous system; useful speculation about pathophysiology and practical attempts at treatment. [Reference]
1821, Sir Charles Bell briefly mentioned a man whose facial nerve was injured by a:
…suppuration which took place anterior to the ear and through which the nerve passed in its course to the face…cases of this partial paralysis must be familiar to every medical observer. It is frequent for young people to have what is vulgarly called a blight; by which is meant, a slight palsy of the muscles on one side of the face, and which the physician knows is not formidable
Bell C. 1821: 21, 25
In 1827, Bell’s classic description was outlined in a case of paralysis of the face on his patient Daniel Stadler.
X. January 2. 1827, Daniel Stalder accompanied his wife, who had a paralytic stroke, to the Middlesex Hospital. It was observed that the left side of his face was much distorted, and there was great wasting of the muscles. He was examined by Mr. Bell, before the pupils of the Hospital, and it proved to be a case of paralysis of the portio dura.
The two sides of his forehead presented a very striking contrast: the right side was furrowed with deep wrinkles, which were more strongly marked when he frowned : a large fold of the skin was prolonged down upon the same side of his nose, which marked the descending slip of the occipitofrontalis muscle; the left side of his forehead was perfectly smooth, the skin appearing to be stretched tightly over the bone, and there was no motion of the integuments in the act of knitting or elevating his eyebrows.
His eyelids were quite motionless. When he was desired to wink, this eye remained open, and the cornea was elevated so as to be quite hid under the upper eyelid. This eye appeared a little duller than the other, yet he says he never had any disease in it. He cannot see so clearly with it as with the other eye. The left nostril is collapsed, and has not that fulness which the right possesses. Some power of acting with his cheeks seems to remain, as in whistling there is a slight quivering observed.
Although his lips are dragged to the right side, yet they do not appear to be totally deprived of muscular power: he can grasp pretty firmly the point of the little finger, when it is introduced into the left angle of his mouth. He states that he has had this affection since he was a child
Bell. Appendix to the papers on the nerves. 1827: 47-50
Associated Persons
- Avicenna [Ibn Sīnā] (980-1037)
- Nicolaus Anton Friedreich (1761-1836)
- François Magendie (1783-1855)
- Sir Charles Bell (1774–1842)
Alternative names
- Idiopathic peripheral facial paralysis
Controversies
It is commonly commented that Bell himself had a right peripheral facial paralysis, however this is erroneous. Bell refers not to himself, but to the physician Professor Roux of Paris who suffered facial paralysis in 1821 [Bell C. 1828 case XVII pp68-70]
References
Original articles
- Afnan SM. AVICENNA [Ibn Sina]: His life (980-1037) and Work. 1958
- Gruner OC. A Treatise on the Canon of Medicine of Avicenna; with translation of the First Book. London: Luzac 1930
- Friedreich NA. De paralysis musculorum faciei rheumatica. Journal der Erfindungen (Gotha), 1797; 8: XXV. Reprint in: Annals of Medicine (Edinburgh) 1800; 5: 214-226.
- Bell C. XXVIII. On the nerves; giving an account of some experiments on their structure and functions, which lead to a new arrangement of the system. Phil. Trans. R. Soc. 1821; 111: 398–424
- Bell C. On the nerves; giving an account of some experiments on their structure and functions, which lead to a new arrangement of the system. London: Bulmer & Nicol. 1821
- Bell C. Case of Paralysis of the Face. In: Appendix to the papers on the nerves. London: Longman 1827:47-50
Review articles
- Bird TD. Nicolaus A. Friedreich’s description of peripheral facial nerve paralysis in 1798. J Neurol Neurosurg Psychiatry. 1979;42:56-58.
- Magendie F. Expériences sur les fonctions des racines des nerfs rachidiens. J. Physiol. Exp. Pathol. 1822; 2: 276–279
- Magendie F. Mémoire sur quelques découvertes récentes relatives aux fonctions du système nerveux. 1823
- Goldman L, Schechter CG. Art in Medicine. Peripheral facial palsy throughout the ages. N Y State J Med. 1967 May 15;67(10):1331-4
- Wilkins RH, Brody IA. Bell’s Palsy and Bell’s Phenomenon. Arch Neurol. 1969;21(6):661-662.
eponymictionary
the names behind the name
Physicianly type with neurological leanings... | LinkedIn |
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |