
![]()
Blue rubber bleb nevus syndrome
Description
Blue rubber bleb nevus syndrome (BRBNS or Bean syndrome) is a rare vascular disorder characterized by multiple venous malformations of varying size and shape, involving most commonly the skin and the gastrointestinal tract, but also the liver, spleen, central nervous system, eyes and heart.
BRBNS patients present typical skin lesions, with some lesions having a rubber-like nipple appearance; the number of skin and GI lesions and the severity of anaemia are correlated. These malformations are a result of mutations affecting angiogenesis, and often result in varying degrees of anaemia and gastrointestinal haemorrhage.

Around 200 cases have been reported in the medical literature.
… we have a spectrum of angiomatous lesions distributed widely throughout the body. I emphasize the fact that in a rare case angiomas of the gut can be inferred with assurance from their presence in the skin. In number, size and location, the vascular lesions may range from the trivial single lesion of the skin or gut to the disastrous destructive angiomatosis when the lesion is almost everywhere. The family history is negative.
Bean, 1958: 183
BRBNS usually occurs sporadically, but it can be inherited as an autosomal dominant trait. A gene mutation has been mapped to the short arm of chromosome 9 and might be involved in these familial cases.
Treatment is dependent on the extent of gut involvement and the severity of the clinical picture. In the absence of massive bleeding, a conservative treatment will be sufficient; otherwise resections are mandatory, but additional lesions may subsequently develop. Management with electrocautery or laser photocoagulation are usually not effective even if some reports recommend them.
Pharmacological treatment with antiangiogenic agents such as corticosteroids, propranolol, interferon-α, octreotide, and sirolimus have been trialled with varying success
History of blue rubber bleb nevus syndrome (Bean syndrome)
Earlier case reports with blue rubber bleb nevus syndrome
1860 – George Green Gascoyen (1829-1876), surgeon to the London Lock hospital, was the first to publish a case. He described a 44-year old patient who had an enlarging parotid gland vascular tumour since birth which eventually suffocated the patient. The patient also had “numerous other naevi scattered over various parts of the body and limbs forming tumours of greater or less size”. Several of these naevi were observed in the intestinal lumen at autopsy. The vessels of the nevi were described to be enormously distended “capillary veins” opening into large pouches, forming true erectile tissue, and that many of the pouches were filled with phleboliths.
1930 – McClure and Ellis recorded longstanding “blood tumors” scattered over the skin of a 30-year old woman who had anaemia, dyspepsia and tarry stools or with bright blood intermittently for the preceding ten years. These blood tumours were also observed in the liver, spleen, stomach, duodenum, jejunum and in the lumen in close proximity to the iliocaecal valve.
1939 – Merchant encountered 2 cases of intussusception of the jejunum due to angiomatous tumours. In one of his cases multiple cutaneous naevi were present.
1947 – Lazarus and Marks described a 58-year old man with nevi on the abdominal skin and multiple small thin walled cavernous capillary angiomas of the colon on colectomy, who had anaemia and gastrointestinal symptoms.
1948 – Holman reported a 9-year old girl with bleeding from an extensive sigmoid cavernous haemangioma, on the background of cutaneous haemangiomas on the hand, suprascapular region, and tongue since 15-months of age.
1951 – Heycock and Dickinson described a 6-year old girl who had 30 red purple angiomas from 2mm to 1cm along the small bowel and colon surgically removed due to recurrent anaemia. The patient also had haemangiomatous lumps of the skin on the chest and spine.
1952 – Rickham described a similar case in a 10-year old boy with a left hand erectile tumour who underwent excision of 3 angiomas resembling “small blackberries” in the small intestine to control intestinal haemorrhage.
1953 – Shepherd described a case with multiple angiomas of the bowel, overgrowth of bone, and congenital dysplastic angiomatosis of the trunk, right arm and leg, along with two non-classical cases with blue angiomas in the ileum and throughout the gastrointestinal tract, but without any cutaneous lesions in his article outlining angiomatous conditions of the gastro-intestinal tract.
1958 – William Bennett Bean (1909-1989) was the first to propose that the syndrome with ‘blue rubber-bleb nevi of the skin and gastrointestinal tract‘ was a distinct entity in his book titled ‘Vascular Spiders and Related Lesions of the Skin‘. He comprehensively presented a case with the blue rubber bleb nevus syndrome along with a brief mention of another case he had seen, and a literature review of pre-existing case reports.
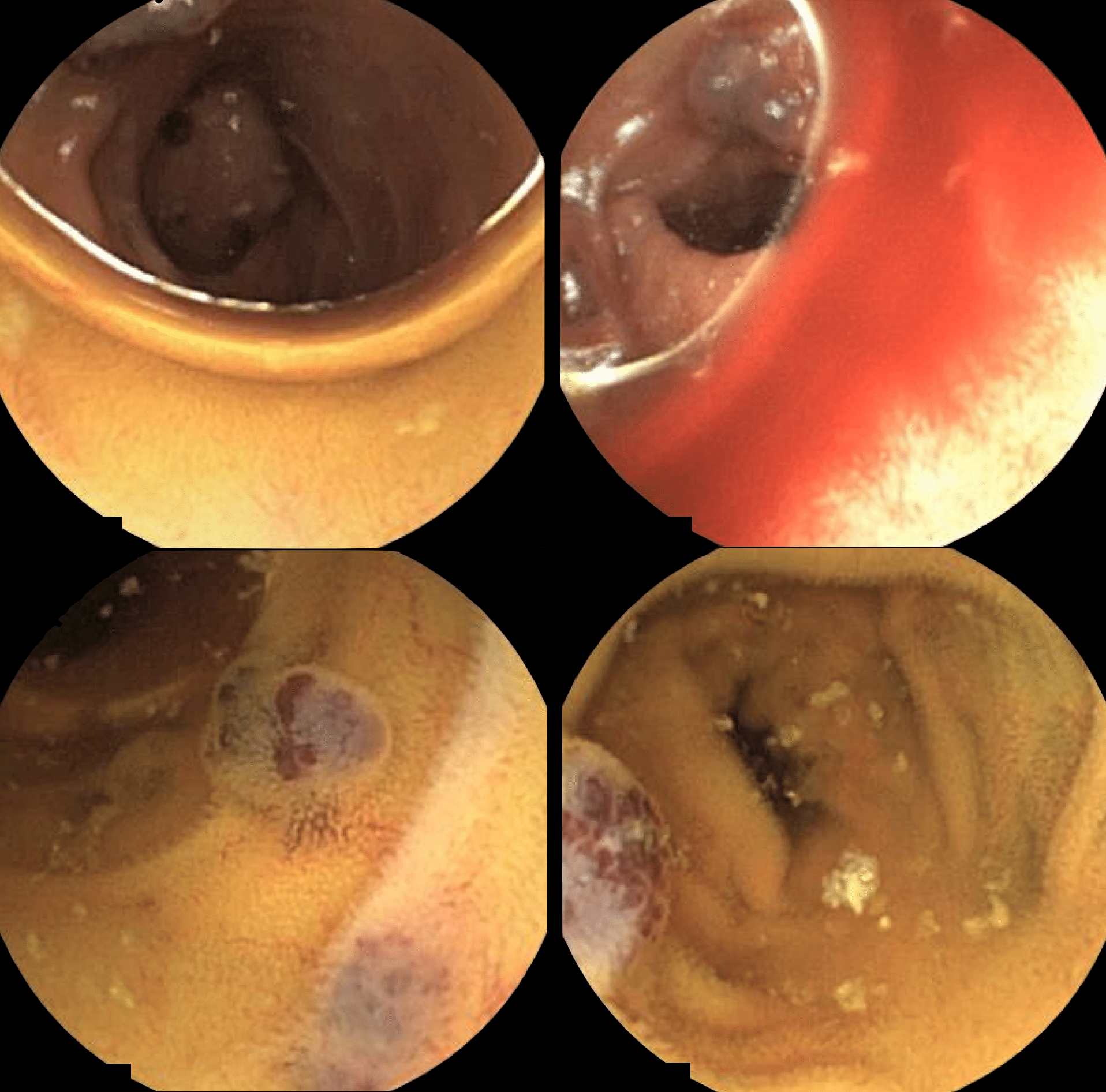
There is a characteristic variety of bluish nevus of the skin found in association with angiomas of the gastrointestinal tract which cause serious bleeding. The larger angiomas have some of the feel and look of rubber nipples, are compressible and refill fairly promptly from their rumpled compressed state. I have called them rubber-bleb nevi though they vary in size, shape and number.
Bean, 1958: 178
While much less common than hereditary hemorrhagic telangiectasia, the syndrome of erectile bluish nevi of the skin and angiomatosis of the gut associated with enteric bleeding is definite.
Bean, 1958 (p179)
Two cases published by Bean
Case 1:
A 3-month old boy who initially presented with a large non-tender haemangioma of the right knee since birth which limited extension at the joint underwent excision of the mass. The patient also had numerous solitary telangiectases on the back, extremities, soles of the feet, and in the parotid regions (Figure 63 – below). Sigmoidoscopy performed for persistent anaemia and bloody stools demonstrated intestinal haemangiomas, which subsequently required a small bowel resection to control the bleeding (Figure 64 – below).
Case 2
A Latin American girl with dark brown skin who had intestinal haemorrhage, anaemia and characteristic lesions of the skin
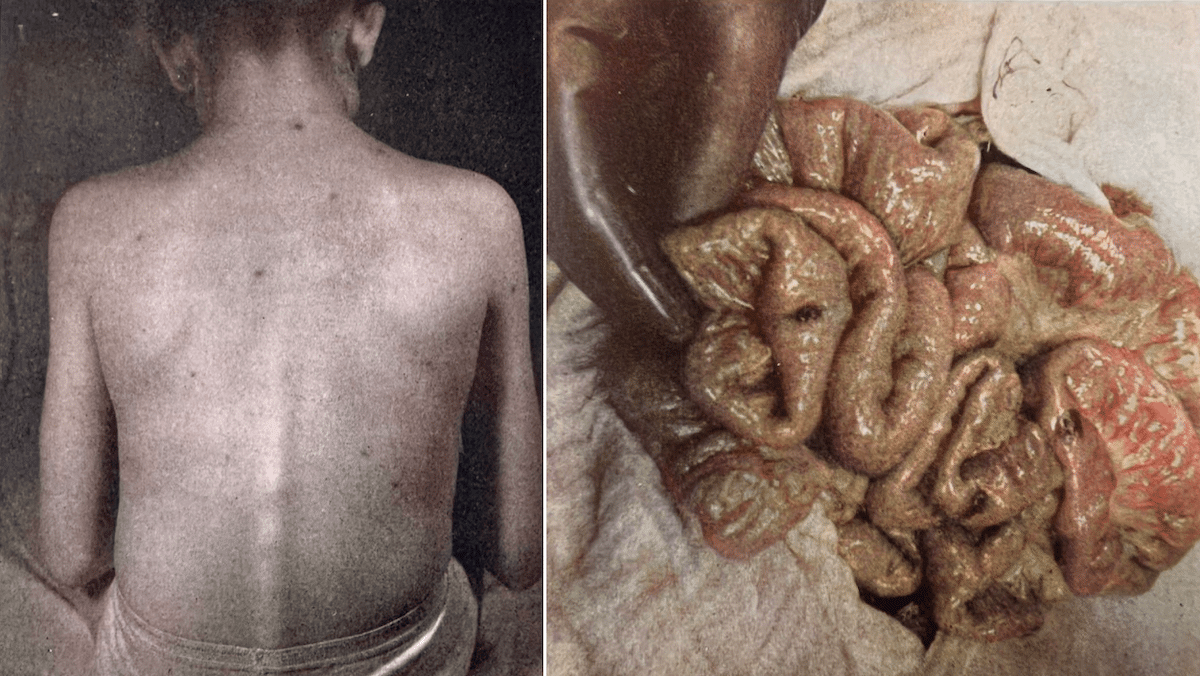
Figure 64 [right]. Blue rubber-bleb nevus. This photograph was taken at operation. It reveals three of the many hemangiomas of the gut of the patient shown in Figure 63.“
Bean, 1958 (p182-183)
The bluish nevi of the skin seen in this syndrome may occur in three main forms.
One is the large disfiguring cavernous angioma which may replace vital structures, or growing too large size, obstruct the airway, alimentary canal, or some other important tubular structure.
Another variety is the blood sac, looking like a blue rubber nipple covered with a milk white tissue of thin skin. These can be emptied of much or all of their contained blood. From the irregular mussed and rumpled state they resume their distended state by the gradual influx of blood.
The third major variety of lesion is the irregular blue mark, sometimes with punctate blackish spots, merging with the adjacent normal skin in a series of color gradations through pale blue to white. Such lesions are elevated above the skin surface only if they are large. The small ones may or may not blanch on pressure. There is rarely complete fading perhaps because of the complex tangle of coiled vascular spaces which trap blood when the structure is compressed.
Bean, 1958: 184-185
Associated Persons
- William Bennett Bean (1909-1989)
Alternative names
- Bean syndrome; Bean’s syndrome
References
Historical references
- Gascoyen GG. Case of Neavus Involving the Parotid Gland and Causing Death from Suffocation: Naevi of the Viscera. Transactions of the Pathological Society of London 1860; 11: 267
- Jaffé RH. Multiple Hemangiomas of the Skin and of the Internal Organs, Archives of pathology. 1929; 7: 44-54
- McClure RD, Ellis SW. Hemangiomata of the Intestine, American Journal of Surgery. 1930; 10: 241-244
- Lazarus JA, Marks MS. Benign intestinal tumors of vascular origin. Surgery. 1947; 22:766.
- Holman CC. Hemangioma of the sigmoid colon: report of a case. Br J Surg. 1948; 36:210.
- Heycock JB, Dickinson TH. Hemangioma of the intestine. Br M J. 1951;1:620.
- Rickham PP. A case of hemangiomatosis of the small intestine. Br J Surg. 1952;39:462.
- Gentry R, Dockerty MB, Clagett OT. Vascular malformations and vascular tumours of the gastrointestinal tract. International Abstracts in Surgery. 1949; 88(4): 281–323
- Shepherd JA. Angiomatous conditions of the gastro-intestinal tract. Br J Surg. 1953 Mar; 40(163): 409-21.
- Aurelius JR, Peterson DH, Niknejad I. Retroperitoneal Cavernous Hemangioma Associated with Hemangiomas of the Skin in a Newborn: Case and Brief Review of Literature, Minnesota Medicine. 1955; 38: 32
Eponymous term review
- Berlyne GM, Berlyne N. Anaemia Due to “Blue Rubber-Bleb” Naevus Disease, Lancet 1960; 276(7163): 1275-1277
- Fine RM, Derbes VJ, Clark WH Jr. Blue rubber bleb nevus. Arch Dermatol. 1961 Nov; 84: 802–805
- Rice JS, Fischer DS. Blue rubber-bleb nevus syndrome. Generalized cavernous hemangiomatosis or venous hamartoma with medulloblastoma of the cerebellum: case report and review of the literature. Arch Dermatol. 1962 Oct;86:503-11.
- Moodley M, Ramdial P. Blue rubber bleb nevus syndrome: case report and review of the literature. Pediatrics. 1993 Jul;92(1):160-2
- Blue Rubber Bleb Nevus Syndrome
- Dòmini M, Aquino A, Fakhro A, Tursini S, Marino N, Di Matteo S, Lelli Chiesa P. Blue rubber bleb nevus syndrome and gastrointestinal haemorrhage: which treatment? Eur J Pediatr Surg. 2002 Apr;12(2):129-33.
- Moser CM, Hamsch C. Successful treatment of cutaneous venous malformations in a patient with blue rubber bleb naevus syndrome by Nd:YAG laser, British Journal of Dermatology, 2012; 166(5): 1143–1145
- Martinez CA et al. Blue rubber bleb nevus syndrome as a cause of lower digestive bleeding. Case Rep Surg. 2014;2014:683684
- Gião Antunes AS, Peixe B, Guerreiro H. Blue Rubber Bleb Nevus Syndrome: A Delayed Diagnosis. GE Port J Gastroenterol. 2017 Mar;24(2):101-103
[cite]
eponymictionary
the names behind the name
Doctor in Australia. Keen interest in internal medicine, medical education, and medical history.
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |