
![]()
Blumberg sign
The Blumberg sign, or more commonly the rebound tenderness test is a clinical sign which may be elicited on physical examination and may be indicative of peritonitis. Deep palpation of the viscera over the suspected inflamed appendix followed by sudden release of the pressure causes the severe pain on the site
History of the Blumberg sign
1907 – Initially described by Jacob Moritz Blumberg (1873-1955), a Polish-German surgeon and gynaecologist. Blumberg believed that pain in the lower abdomen after abrupt withdrawal of the hand from the lower abdominal quadrant was a sign of appendicitis.
Blumberg believed that pain in the lower abdomen after abrupt withdrawal of the hand from the lower abdominal quadrant was a sign of appendicitis. Performed by gradually increasing the pressure of the palpating hand over the tender spot, and then removing abruptly. If the patient winces with pain upon withdrawal of the hand, the test is positive indicating a likelihood of peritonitis
Original
English
Zunächst einen Druck auf die zu untersuchende Stelle des Abdomens auszuüben und den Patienten zu fragen, ob es schmerzt, dann nach erhaltener Antwort die palpierende Hand plötzlich abzuheben und nun sich von dem Patienten sagen zu lassen, ob im Moment des Abhebens es geschmerzt habe, resp welcher Schmerz grösser gewesen sei.
Die Methode lässt sich mit grösster Exaktheit anwenden, da es sich ja nicht um die Beurteilung der Grösse eines Schmerzes handelt, sondern um den Vergleich der Intensität zweier Schmerzen, und diese Angabe wird von den Patienten sehr zuverlässig gemacht.
1907; 54: 1177-1178
First of all exert pressure on the area of the abdomen to be examined and ask the patient whether it hurts, then suddenly raise the palpating hand after receiving the answer and now let the patient tell you whether it hurt at the moment of lifting off or what pain was greater.
The method can be used with the greatest accuracy, since it is not a matter of assessing the size of one pain, but of comparing the intensity of two pains, and this information is very reliably given by the patient.
1907; 54: 1177-1178
1970 – WG Prout determined that the demonstration of rebound tenderness suffers the twin disadvantages of being both unpleasant for the patient and of being diagnostically useless.
The physical sign of rebound tenderness has been studied in 100 patients with acute abdominal pain. In the majority of cases this sign proved unhelpful and was actually misleading in many instances. There seems little justification for the use of a sign which relies on causing a sudden and unexpected pain in a patient in whom confidence in the gentleness of the examining hand is vital.
Prout WG, 1970
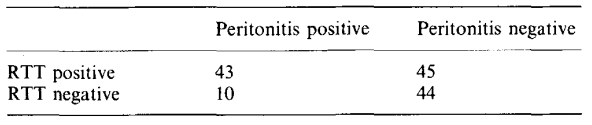
1991 – Liddington and Thomson investigated the usefulness of the rebound tenderness test in indicating peritonitis. They prospectively assessed the sign in 142 unselected patients admitted as emergencies with abdominal pain and tenderness. It was found to be of no predictive value. [Sensitivity 0.81; Specificity 0.49]

Liddington, Thomson 1991
Liddington, Thomson 1991
Associated Persons
- Jacob Moritz Blumberg (1873 – 1955)
- Dmitri Sergeevich Shchetkin (1851–1923)
References
Original articles
- Blumberg, JM. Ueber ein neues diagnostisches Symptom bei Appendicitis. Münchener medizinische Wochenschrift, 1907; 54(1): 1177-1178
Review articles
- Prout WG. The significance of rebound tenderness in the acute abdomen. Br J Surg. 1970; 57(7): 508-10.
- Liddington MI, Thomson WHF. Rebound tenderness test. Br J Surg. 1991; 78(7): 795-6.
- Eponymythology: Appendicitis eponymous signs. LITFL
eponymictionary
the names behind the name

MBBS BSc (Hons), Imperial College London. Emergency trainee with an interest in research and all things surgical
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |