
![]()
Clavicle fractures
Clinical case
Clavicle fractures:
- Are common childhood fractures, that also affects adult patients as well.
- Can result in neonates from birth trauma, and generally sustained in later age from sporting injuries, falls and violence.
- The clavicles superficial location, its thin midshaft, and the forces transmitted across it makes the clavicle a common site of injury.
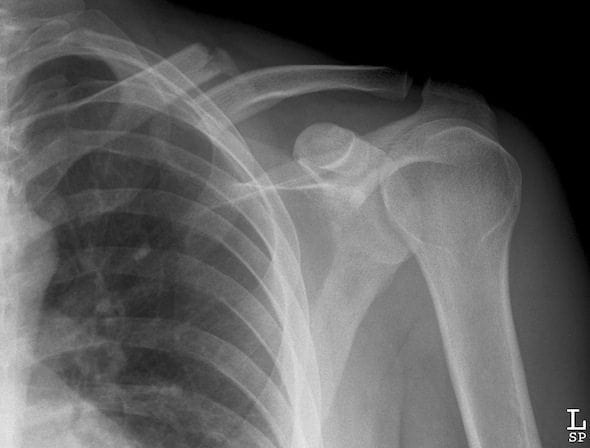
16 year old boy arrives at triage holding his left arm adducted close to his chest and supporting it with his right hand. He sustained an injury to his left shoulder during a ‘wrestling’ encounter with his older brother
On examination he was moderately distressed with a pain score 5/10. Palpation revealed pain over clavicular region, and limited range of movement for the left shoulder, in particular he was unable to actively abduct his left arm. He was given oral analgesia and sent for X-ray…


Anatomy:


Types of Clavicle Fractures:
- Proximal Clavicle Fractures [Type A]
- Occurs in 5% of clavicle fractures making it a very uncommon injury to treat
- The proximal clavicle fracture tends not to displace related to good ligamentous support.
- Displaced proximal fractures require close examination for neurovascular compromise, and generally require reduction.
- Nondisplaced proximal fractures are treated with sling for comfort, analgesia, and range of movement exercises when pain allows.
- Midshaft Clavicle Fractures: [Type B]
- Occurs in 80% of clavicle fractures, making it the most common type off fracture.
- Diagnosis of midshaft clavicle fractures is generally straight forward based on history, examination and radiology.
- Treatment of midshaft clavicle fractures involves restore normal anatomy, limit pain, and promote quick return to activity or play.
- Distal Clavicle Fractures: [Type C]
- Occurs in 15% of clavicle fractures
- Distal clavicle fracture occurs distal to the coracoclavicular ligaments.
- Divided into 3 types nondisplaced, displaced and articluar.
- Displaced distal clavicle fractures tend to require internal fixation for support.
“Types of Clavicle Fractures”
Assessment of Clavicle Fractures:
- Patients generally present with pain and swelling over the area and report a history of trauma or fall onto the area.
- Children not presenting with a history of trauma should be evaluated for malignancy, rickets, and non-accidental injury.
- Severe displacement can cause tenting of the skin and ecchymosis.
- Assess for tenderness, crepitus, oedema, deformity, and decreased pulse and perfusion distal from the injury.
- An anteroposterior X-ray of the shoulder usually shows the fracture clearly.
- Occasionally, special views will be required to delineate medial clavicle injuries.
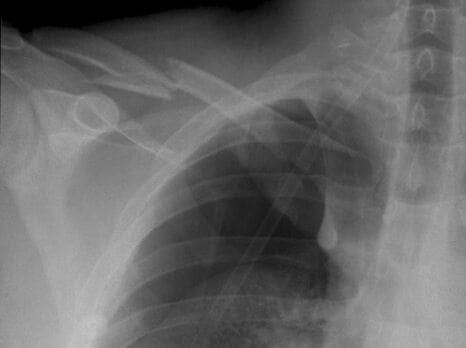
- Chest X-ray is indicated if pneumothorax is suspect
- Look for associated local injuries such as gleno-humeral dislocation, scapula and rib fractures and potential intrathoracic injury such as
- Pneumothorax
- Subclavian artery and vein injury
- Internal jugular vein injury
- Axillary artery injury


Management of clavicle fractures.
- Support the weight of the arm in a triangular sling, and give an analgesic such as paracetamol/codeine preparations, or NSAIDs.
- The traditional figure-of-eight bandage has generally been abandoned, as it is uncomfortable and difficult to keep tight.
- Refer the patient to the next Fracture clinic, for follow up X-rays and further management.
- Displaced or communited fractures, and fractures with more than 15 to 20mm clavicle shortening, should be referred immediately to the orthopaedic surgeon, for operative management to prevent nonunion.
Complications of Fractured Clavicles:
- Fractures of the middle third of the clavicle have been associated with injuries to the neurovascular bundle.
- Brachial plexus compression resulting from hypertrophic callus formation
- Delayed union or nonunion
- Poor cosmetic appearance
- Post-traumatic arthritis
Reference:
- Benjamin, H. & Hang, B. (2007). Common Acute Upper Extremity Injuries In Sports. Clinical Paediatric Emergency Medicine. 8, 15-30.
- Kim, W. & McKee, M. (2008). Management of Acute Clavicle Fractures. Orthopaedics Clinics of North America. 39, 491-505.
- Pecci, M. & Kreher, J. (2008). Clavicle Fractures. American Family Physician. 77(1), 65-70.
[cite]
Emergency nurse with ultra-keen interest in the realms of toxicology, sepsis, eLearning and the management of critical care in the Emergency Department | LinkedIn |