
![]()
Collapse and recruit
aka Pulmonary Puzzler 009
A 19 year old male is admitted after a severe traumatic brain injury. Due to refractory intracranial hypertension he has been intubated and is receiving 20mg an hour of morphine, 20mg an hour of midazolam and 200mg an hour of propofol. He is paralysed for intracranial pressure control.
You are called to the bedside because he has desaturated to the mid 80s on 100% oxygen.
A chest X-ray is obtained.
Questions
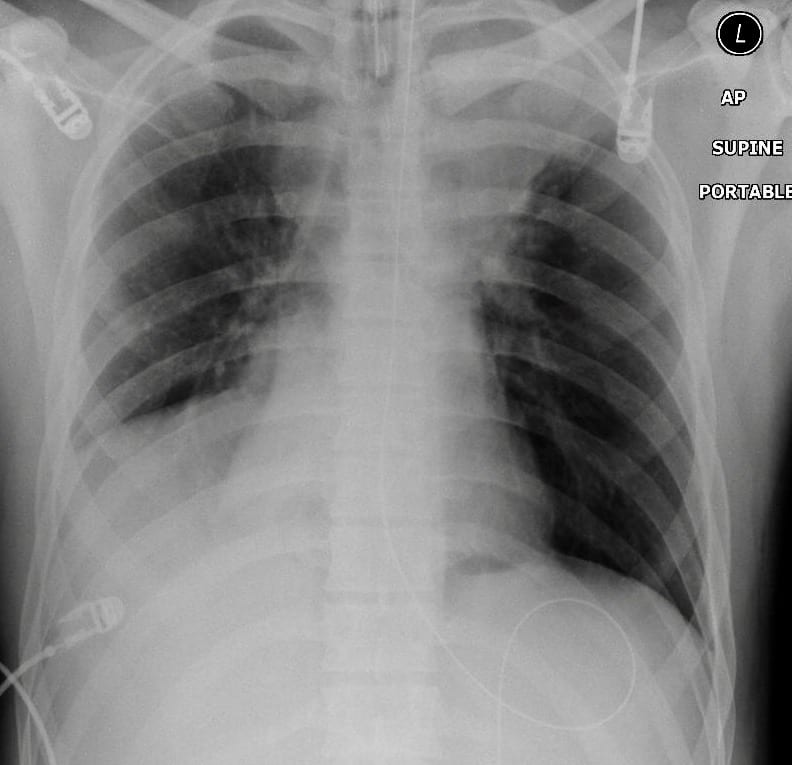
Q1. Describe the chest X-ray findings.
Answer and interpretation
There is collapse of the left upper lobe, the right middle lobe and the right lower lobe.
Q2. Why is the patient hypoxic despite administration of 100% oxygen?
Answer and interpretation
Deoxygenated blood is being shunted through the collapsed areas of lung. This shunted blood is not exposed to the oxygen that the patient is breathing in.
Q3. Why has this happened?
Answer and interpretation
This has happened because the patient is unable to cough (he is paralysed) and the left upper lobe bronchus and bronchus intermedius are blocked with sputum plugs.
Q4. How can you fix the problem?
Answer and interpretation
The options are to:
- perform a bronchoscopy and remove the plugs
- attempt to reinflate the lungs using recruitment maneuver
Q5. You decide to have a go at the second option to fix the problem. Describe how you will proceed and outline any complications that might be expected.
Answer and interpretation
One commonly described technique is to apply 40cmH20 of PEEP for 40 seconds. This technique is often poorly tolerated for two reasons. Firstly, during the manoeuvre, the size of West Zone 1 is increased and the patient often desaturates as a consequence of this. Secondly, the prolonged application of high PEEP significantly reduces venous return and significant hypotension often results.
An alternative method is to change the patient to a pressure controlled mode of ventilation, to increase the PEEP to 20cmH20 and then to apply Pressure Control at 20-30cmH20 above PEEP for 5 breaths. This method is generally better haemodynamically tolerated and provides effective recruitment.
Complications of recruitment maneuvers include:
- pneumothorax
- hypotension
- hypoxia
- raised intracranial pressure
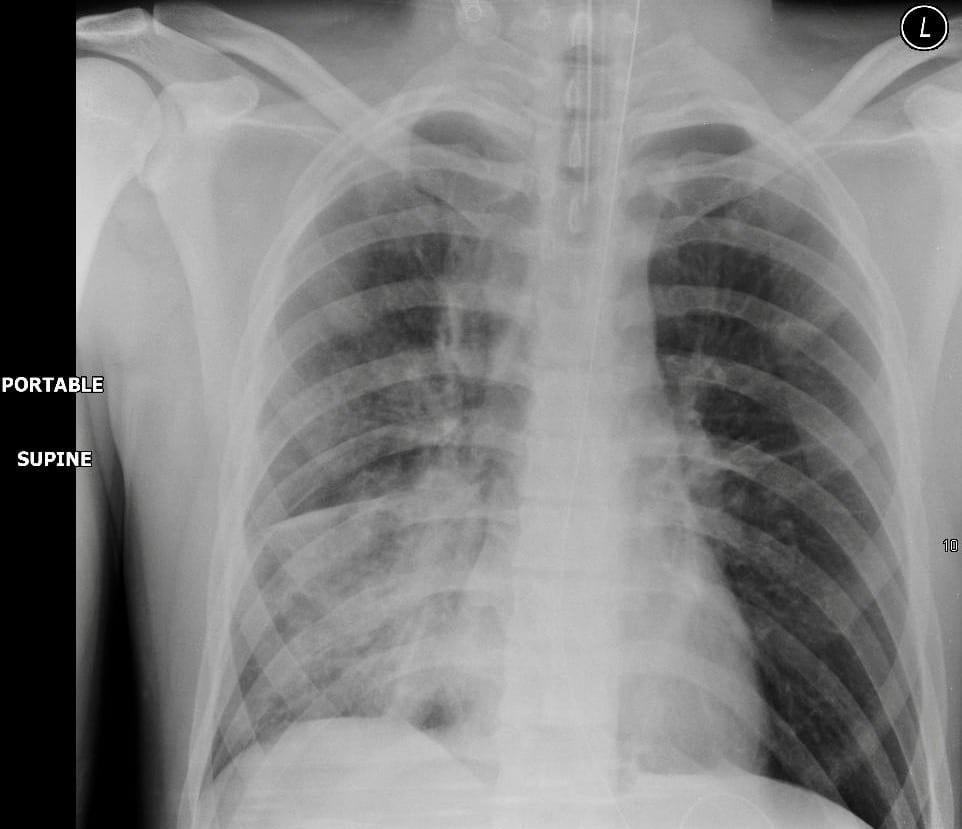
Q6. Describe the post-maneuver chest X-ray
Answer and interpretation

- The chest X-ray shows resolution of the left upper lobe collapse.
- The right middle and lower lobe collapse is persistent.
Q7. What will you do now?
Answer and interpretation
It depends on the clinical condition of the patient.
The intervention that is likely to be required to improve the right sided collapse is a bronchoscopy; however, given that the patient has raised intracranial pressure, this is may be poorly tolerated.
In this instance a bronchoscopy was able to be safely performed and the following chest X-ray showing improved expansion of the right base was obtained after the procedure:
References
- For more Pulmonary cases check out the LITFL Top 150 Chest X-Rays

CLINICAL CASES
Pulmonary Puzzler
Intensivist in Wellington, New Zealand. Started out in ED, but now feels physically ill whenever he steps foot on the front line. Clinical researcher, kite-surfer | @DogICUma |