
![]()
Could it be renal colic?
aka Metabolic Muddle 001
Consider a 65 year-old male presenting with right-sided flank pain radiating to the groin.
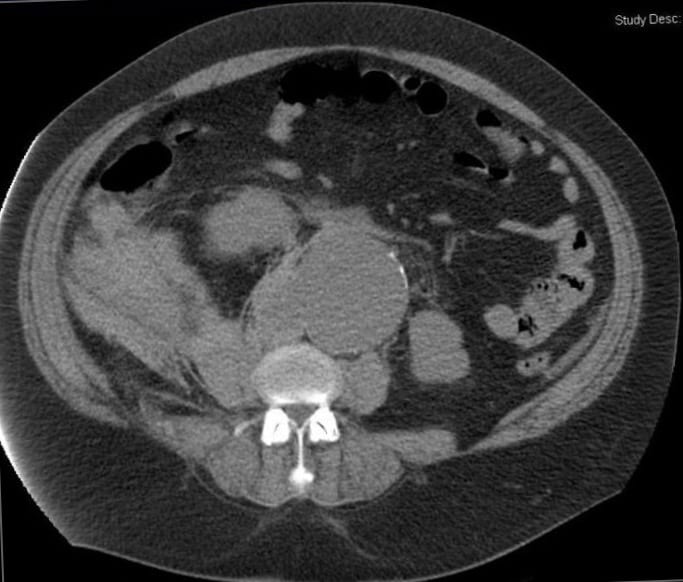
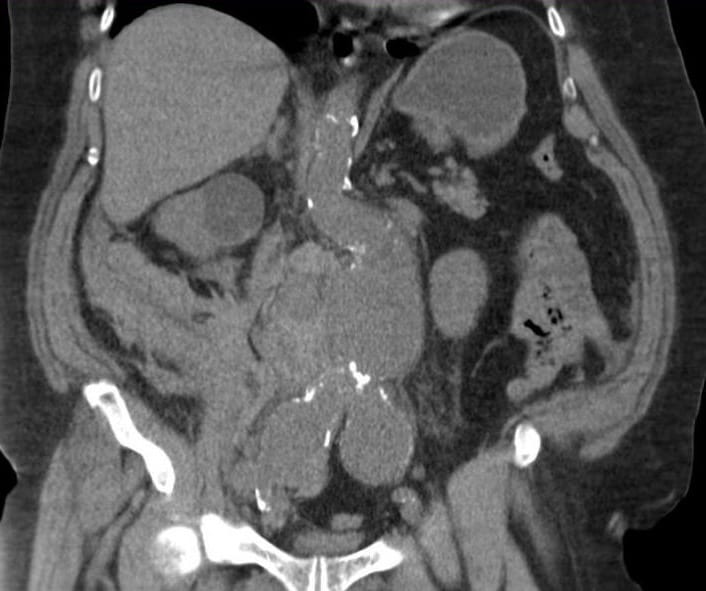
The following CT scan was taken to confirm a presumed diagnosis of renal colic:
Questions
Q1. Describe the CT scan
Answer and interpretation
CT scan is non-contrast; however, there is:
- right-sided retroperitoneal blood evident
- an abdominal aortic aneurysm
It is important to remember that the commonest cause of the ‘classic’ presentation of renal colic among patients presenting to have a post-mortem is ruptured abdominal aortic aneurysm.
This patient needs an emergency AAA repair.
The patient was taken to theatre for emergency surgery. The following biochemistry results were taken post-operatively:
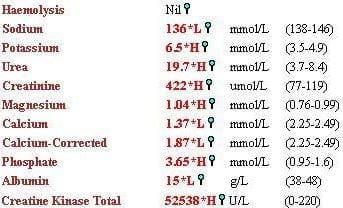
Q2. Describe the biochemistry. What diagnosis is suggested by these biochemical findings?
Answer and interpretation
Biochemistry demonstrates acute renal failure with a reduced urea-to-creatinine ratio.
The likely diagnosis is rhabdomyolysis in this clinical context.
Features suggestive of this diagnosis are:
- increased urea and creatinine with a reduced urea-to-creatinine ratio
- hyperphosphataemia, hypocalcaemia, hyperkalaemia
- metabolic acidosis
- increased CK (usually to greater than 40,000)
- Although not measured here, AST, and LDH are also increased in rhabdomyolysis
Q3. What are the other potential causes of renal failure to consider in this clinical situation?
Answer and interpretation
Other potential causes:
- hypovolaemia from bleeding
- renal artery occlusion during operation
- use of contrast in pre-operative CT scan (not in this case)
- use of nephrotoxic drugs like gentamicin
- low cardiac output from peri-operative myocardial infarction
- abdominal compartment syndrome
CLINICAL CASES
Metabolic Muddle
Intensivist in Wellington, New Zealand. Started out in ED, but now feels physically ill whenever he steps foot on the front line. Clinical researcher, kite-surfer | @DogICUma |
I don’t understand why the rhabdo happened?