
![]()
Evan O’Neill Kane
Evan O’Neill Kane (1861-1932) was an American general surgeon
Kane was a ‘country surgeon’ based in Kane and spent three decades as chief surgeon at Kane Summit Hospital (an outgrowth of the cottage hospital founded by his mother, Elizabeth Wood Kane).
Kane became internationally famous in 1921 when he performed an auto-appendicectomy to demonstrate both the feasibility of appendicectomy under local infiltration and the patient experience of the operation.
Kane was retained by multiple railroads and wrote from hard-won experience about shock, field improvisation, and the realities of accident medicine. Kane designed or promoted practical solutions for austere environments such as rapid hypodermoclysis for shock, fire-proof asbestos dressings, an acetylene headlight for night operations, and even mica as a transparent cranial “window”). He also embraced comfort innovations such as use of the phonograph in the operating-room.
Biographical Timeline
- Born on April 6, 1861 in Darby, Pennsylvania (USA) son of American Civil War Major General Thomas L. Kane, the founder of the town Kane, Pennsylvania
- 1884 – Graduated Jefferson Medical College (Philadelphia) (MD).
- 1887 – With his mother (Elizabeth Dennistoun Wood Kane) and brother, helped found Woodside Cottage Hospital in Kane, Pennsylvania (later Kane Summit Hospital).
- 1892 – Hospital moved to a larger site and became known as Kane Summit Hospital.
- Late 19th–early 20th century – Served as chief surgeon at Kane Summit Hospital and worked as a railway surgeon for multiple railroads
- 1921 (15 Feb) – Performed a highly publicised self-appendicectomy under local anaesthesia, later publishing the case as “Autoappendectomy: a case history”
- 7 Jan 1932 – Performed self-inguinal hernia repair under local anaesthesia
- Died on April 1, 1932 in Kane, Pennsylvania, aged 70.
Key Medical Contributions
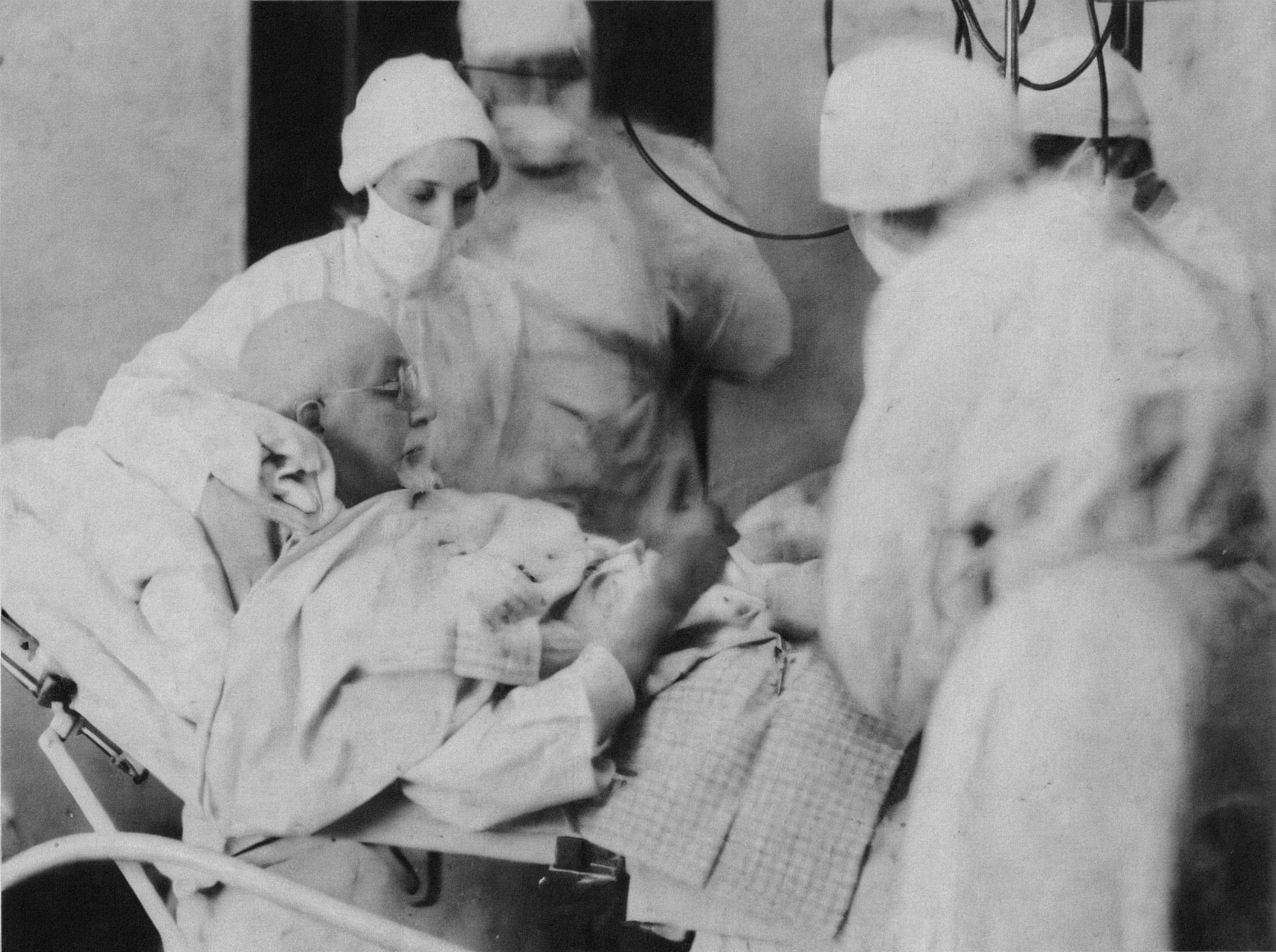
Auto-appendicectomy (February 15, 1921)
Kane published his own case report, and it reads like a deliberate proof-of-concept for major abdominal surgery under local anaesthesia. He describes chronic appendicitis, minimal prep (“one day’s starvation” and oil), walking to hospital, premedication with morphine, then announcing (to everyone’s alarm) that he would perform the operation himself.
He positioned himself semi-sitting with the table head raised, pillows under his shoulders, a foot brace to flex hips/knees, and had the anaesthetist push his head forward so he could see the field.
Technique details from the primary report:
- Incision planning: mapped the site “one inch below McBurney’s point,” planned a 3.5 inch diagonal incision (larger than he preferred in routine cases because he “did not know what to expect” in himself).
- Local anaesthesia: infiltrated locally with “cocain and adrenalin” (not novocaine as frequently quoted) into skin and deeper abdominal wall. Kane noted the striking the peritoneum produced a “sharp prick” sensation. He then waited ~4 minutes before incision.
- Finding the appendix: Kane reports no adhesions and lifting the caecum exposed the appendix. It appeared enlarged/injected with concretions. He then had an assistant hold it up under tension while he ligated in the usual way.
- Closure: Kane states he left wound closure to his assistants
Kane explicitly framed the self-operation as evidence that local anaesthesia could be tolerated for “major operation” and therefore might spare patients in whom general anaesthesia was risky.
His advocacy for the exclusive local anaesthetic in procedures predated his autoappendicectomy. Nine years prior to this operation, he performed an appendicectomy on his then nine-year-old son, Robert, using only local anaesthetic.
Historical inconsistencies of the 1921 operation and re-telling
Local anaesthetic used (cocaine vs novocaine/procaine)
Kane’s own case report states he injected “cocain and adrenalin” locally (after a pre-op morphine injection). Many secondary retellings substitute novocaine/procaine, often implying it was chosen as a “safer” agent.
How he could see what he was doing (mirrors vs positioning)
In the primary description, Kane does not mention mirrors; instead he describes positioning (cross-brace for feet, table adjustments, pillows, “doubling” himself up) and instructing the anaesthetist to push his head forward to get “a fairly good view.”
“Painless” vs candid discomfort
Kane is explicit that the procedure was not uniformly painless: he reports “some discomfort” when tightening the mesenteric ligature (because he didn’t wait for anaesthetic effect) and pain with some peritoneal and some skin stitches outside the anaesthetised field. He also made interesting observations on the types of pain experienced. He confirmed that pain during manipulation of the intestines and appendix was referred to the umbilicus or even to the left; that pain was greater when intestines were returned to the abdomen rather than when traction was applied to them; and that these pains were similar to the colicky pain experienced with acute appendicitis.
Auto-hernia repair (January 7, 1932) — the second public “self-operation”
Kane operated on himself again for an inguinal hernia on January 7, 1932, following a horseback riding injury. Contemporary press descriptions emphasised his composure as he “smiled throughout,” and “joked with the nurses”.
The operation was performed at Kane Summit Hospital under local anaesthesia, with press present, and was regarded as riskier than the appendectomy because of potential vascular damage. The operation reportedly took as 1 hour 55 minutes with Kane “back operating” 2 days later.
Key medical contributions (beyond the self-surgery headlines)
Railway surgery innovations (shock and austere operating).
Kane devised equipment and methods intended for emergency/field conditions including rapid hypodermoclysis concepts and other practical aids emerging from railway trauma work. Accounts of his innovations highlight materials and practicality such as:
- Fire-proof asbestos surgical dressings that could be rapidly sterilised over open flame (in the era before sealed sterile packs).
- Acetylene headlight for night operating and field illumination.
Early patient-centred workflow ideas.
In the hospital setting he proposed:
- using a phonograph/music pre-anaesthesia to calm patients.
- advocating newborn tattoo identification (paired marks for infant and mother) to prevent mix-ups in small hospitals.
Innovations in general surgical equipment.
He modified and invented various surgical tools:
- Widening the aperture of the Murphy button (a device used for intestinal anastomosis prior to the advent of end-to-end stapling) to reduce post-operative obstruction of the anastomosis.
- Intra-abdominal ligating clips. He unsuccessfully trialled aluminium ligating clips in around 1900 (over half a century before Ernest C Wood’s patent in 1968), but was limited by their irritant and fibrosing effect on surrounding tissue.
Major Publications
- Kane EO. Fire-proof asbestos surgical dressing. JAMA 1895;XXV;(23):996-997.
- Kane EO. Simple device for rapid hypodermoclysis in combating shock. American Academy of Railway Surgeons 1900: 31-34
- Kane EO. A new coupler for rapid intestinal anastomosis. JAMA. 1902;xxxviii(16):1003–1005.
- Kane EO. Acetylene headlight and reflector for night operating. JAMA 1904;XLIII;(17):1231.
- Kane EO. Cardiac dilatation and displacement due to pleurisy. JAMA 1911;LVII;(10):792-793.
- Kane EO. The Army Canteen. JAMA. 1912;LVIII(5):363.
- Kane EO. Phonograph in Operating-Room. JAMA 1914;LXII;(23):1829.
- Kane EO. Absorbable metal clips as substitutes for ligatures and deep sutures in wound closure. JAMA. 1917;LXIX;(8):663-664.
- Kane EO. Case History of Centenarian — Cancer — Radium. Buffalo medical journal. 1917; 72(1): 13
- Kane EO. Bullet in Brain Destroying Sight and Hearing — Recovery. Buffalo medical journal. 1917; 72(10): 455-458
- Kane EO. Autoappendectomy.(A case history). The International journal of surgery. 1921; 34(3): 100-102.
- Kane EO. Tattooing new born infants for permanent identification. Proceedings of the Pennsylvania Academy of Science. 1931; 5: 74-75
References
- DR. EVAN KANE DIES OF PNEUMONIA AT 71; Surgeon Who Operated Twice on Himself Fails to Rally Under Oxygen Tent. CUT OUT HIS OWN APPENDIX Navel Achievement Drew Nation-Wide Attention — Aided in Acquittal of Son on Murder Charge. April 2, 1932 New York Times
- Rennie D. Do It to Yourself Section: The Kane Surgery. JAMA. 1987;257(6):825–826.
- Sasson M, Shvartzman P. Hypodermoclysis: an alternative infusion technique. Am Fam Physician. 2001 Nov 1;64(9):1575-8.
- Nwaogbe C, Simonds EA, D’Antoni AV, Shane Tubbs R. Surgeons performing self-surgery: A review from around the world. Translational Research in Anatomy 2018; 10: 1-3
- Radhakrishnan J, Koo N. Atypical appendectomies. Hektoen International 2021
- Dr. Evan O’Neill Kane: The surgeon who operated on himself three times Jerusalem Post, 2022
- Cadogan M. Auto-appendicectomy. LITFL
Eponym
the person behind the name

DM (UWA), BM (Indiana), FMusA, LMusA. Resident Medical Officer, Sir Charles Gairdner Hospital. Basic Surgical Streaming Program. Professional violinist, now aspiring surgeon. Loves music, opera, and operating.
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |