
![]()
First disease
Measles, rubeola
Measles, also known as rubeola or “First Disease,” is a highly contagious viral illness with a distinctive maculopapular rash, fever, and prodromal symptoms of cough, coryza, and conjunctivitis. Caused by a single-stranded, negative-sense RNA virus of the Morbillivirus genus, it is transmitted primarily via airborne droplets and has a basic reproduction number (R0) among the highest of all infectious diseases.
Before the introduction of vaccination, measles was nearly ubiquitous in childhood; infection was nearly universal by adolescence. Though commonly self-limiting, complications such as otitis media, pneumonia, encephalitis, and subacute sclerosing panencephalitis (SSPE) account for significant morbidity and mortality, particularly among malnourished and immunocompromised individuals.
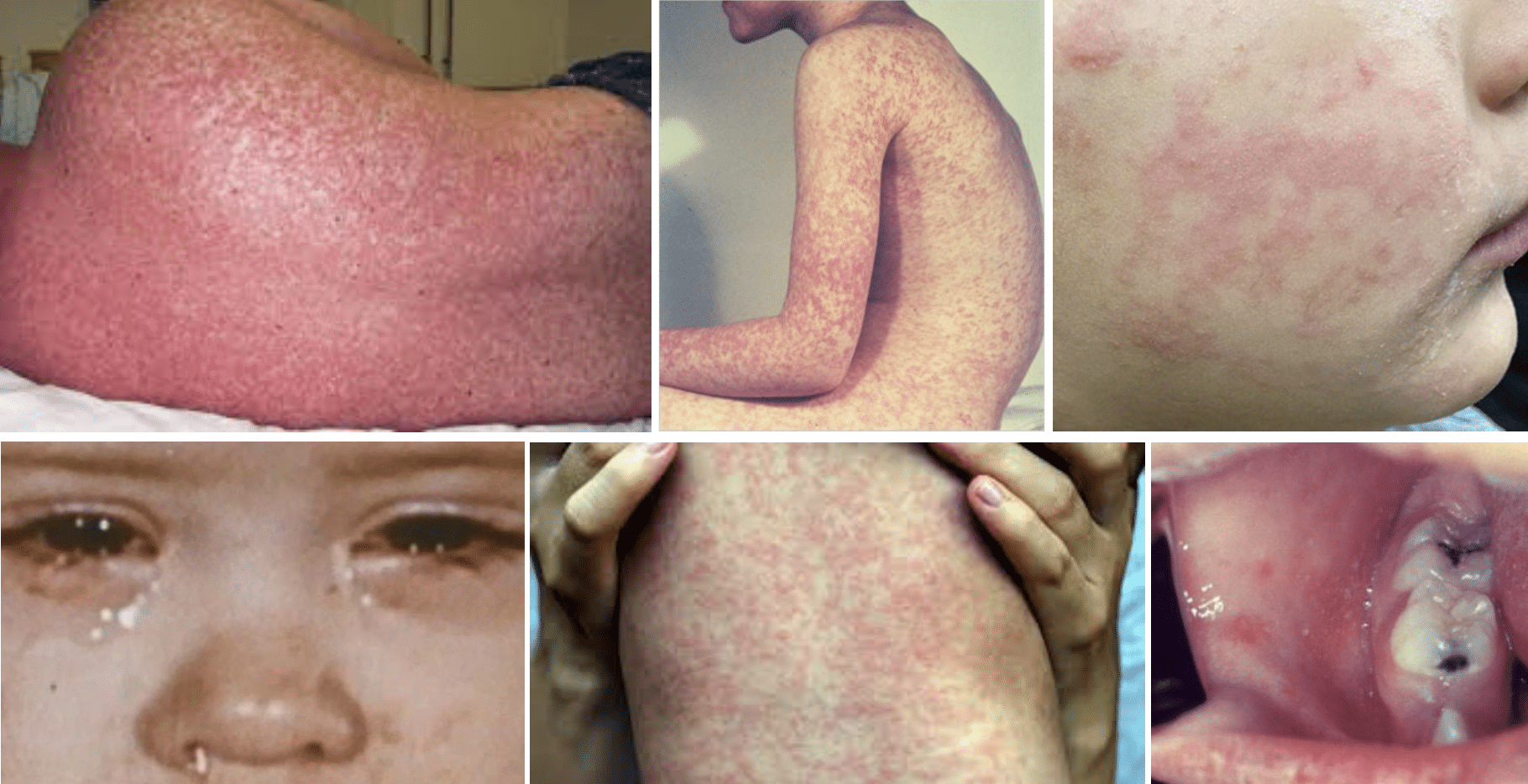
The disease’s signature rash typically begins at the hairline, spreading cephalocaudally, and may “stain” or darken before resolving. Koplik spots—small white lesions with erythematous halos on the buccal mucosa—are pathognomonic. Measles induces profound immunosuppression, termed “immune amnesia,” which predisposes to secondary infections.
Measles is “First Disease” among the six classical childhood exanthems, a term coined in the early 20th century to streamline the differential diagnosis of febrile rashes. Its classification underscores both its ancient recognition and foundational place in pediatric infectious disease education.
Since the introduction of a live attenuated vaccine in 1963 (and its improved versions thereafter), global incidence has plummeted. However, outbreaks continue to recur, particularly in settings of declining immunisation coverage due to vaccine hesitancy or systemic access barriers. Notably, measles was declared eliminated from the United States in 2000, though this status has faced repeated threats from imported cases and domestic undervaccination.
Synonyms of first disease: Rubeola, Measles, Hard measles, 14‑day measles, Morbilli, Sarampión
English physician Clement Dukes (1845–1925) introduced the numbering system for childhood exanthems in 1900. He categorised them by clinical presentation into: First: measles; Second: scarlet fever; Third: rubella; and Fourth: Filatov-Dukes disease. Later additions – Fifth: erythema infectiosum (1905, Cheinisse); and Sixth: roseola infantum (1910, Dreyfus)
Clinical Manifestations
Incubation and Prodrome
- Incubation period: 7–14 days post-exposure (mean ~10 days).
- Prodromal symptoms: High-grade fever (up to 40.6°C), malaise, cough, coryza, conjunctivitis — the “3 Cs”.
- Koplik spots (enanthem): Small bluish-white lesions with red halos on the buccal mucosa opposite molars. Pathognomonic, appearing 1–2 days before rash.
Exanthem Phase
- Rash (exanthem) onset: Typically 3–5 days after prodrome begins. Starts behind ears/hairline and spreads cephalocaudally.
- Rash description: Erythematous maculopapular, becoming confluent in places; may desquamate in recovery.
- Rash fades in the order it appeared, leaving a brownish staining or fine peeling.
Diagnosis
Clinical Diagnosis
- Diagnosis is often clinical in endemic areas based on:
- Prodrome with 3 Cs
- Koplik spots
- Cephalocaudal rash progression
- Consider measles in any patient with febrile rash illness and recent travel or exposure.
Laboratory Confirmation
- Serology: Measles-specific IgM antibodies (detectable ~3 days after rash onset).
- PCR: Detection of measles RNA from nasopharyngeal, throat, or urine specimens (ideal early in illness).
- Other labs: Leucopenia, thrombocytopenia, raised CRP; consider CXR if pneumonia suspected.
Differential Diagnosis
- Rubella
- Roseola (HHV-6)
- Erythema infectiosum (Parvovirus B19)
- Scarlet fever
- Drug hypersensitivity reactions
- Dengue, Zika, and other viral exanthems
Complications
Measles is not benign — up to 30% of cases develop complications, with higher risk in children <5, adults >20, the malnourished, and the immunocompromised.
Common Complications
- Otitis media – most frequent complication in children; may lead to permanent hearing loss.
- Pneumonia – leading cause of measles-associated death; due to virus itself or secondary bacterial infection.
Severe/Long-Term Complications
- Acute encephalitis (~1 in 1,000) – fever, seizures, altered mental status; 15% mortality, 20–40% with neurological sequelae.
- Subacute sclerosing panencephalitis (SSPE) – rare but fatal neurodegenerative disease appearing 7–10 years post-infection.
- Blindness – especially in vitamin A-deficient populations or those with corneal ulceration.
- Deafness – secondary to measles-associated otitis or auditory nerve involvement.
Pregnancy-Related Risks
- Miscarriage
- Premature labour
- Low birth weight
- No clear congenital measles syndrome, but fetal risks are significant.
Immunological Effects
- “Immune amnesia” – transient but profound immunosuppression lasting weeks to months. Increased susceptibility to other infections.
Treatment
- Supportive care: Hydration, antipyretics, vitamin A supplementation.
- Isolation: To prevent transmission.
History of first disease – measles
c. 340 CE – Ko Hung (Ge Hong) Chinese alchemist reportedly distinguishes measles from smallpox in early medical texts. One of the earliest recorded clinical differentiations of rash illnesses.
c. 640 CE – Ahrun (Aaron) the Christian Priest. Egyptian cleric provides further differentiation of measles and smallpox in early Arabic texts, a topic explored in Greco-Arabic medical traditions.
910 CE – Abu Bakr Muhammad ibn Zakariya al-Razi (Rhazes) (c.865–925) Persian polymath and physician. Authored Kitab fi al-jadari wa al-hasbah (“Treatise on Smallpox and Measles”), regarded as the first definitive clinical description of measles and differentiation from smallpox.
The eruption of measles is preceded by a continued fever, pain in the back, itching in the nose and sneezing…
Rhazes
1757 – Francis Home (1719–1813) Scottish physician. Demonstrates that measles is caused by a transmissible agent in the blood of infected patients. First attempt at immunisation using blood from infected individuals.
Considering how destructive this disease is, considering how many die…I thought I should do no small service to mankind, if I could render this disease more mild and safe, in the same way as the Turks have taught us to mitigate the small-pox
1846 – Peter Ludwig Panum (1820–1885) Danish physician. Investigated a measles outbreak in the Faroe Islands, noting its extreme contagion and lifelong immunity after infection.
…it is quite remarkable that of the many old people still living on the Faroes who had had the measles in 1781, not one, was attacked the second time. I myself saw 98 such old people, who were exempt
1896 – Henry Koplik (1858-1927) American pediatrician. Describes bluish-white buccal lesions (now “Koplik spots“) in Archives of Pediatrics, confirming them as an early diagnostic sign.
1912 – Measles becomes nationally notifiable in the USA. U.S. health authorities begin systematic case reporting. ~6,000 deaths annually reported in the pre-vaccine era.
1954 – Thomas C. Peebles (1921–2010) and John F. Enders (1897–1985). Peebles isolates the measles virus from 11-year-old David Edmonston in Boston. Enders, who previously shared the Nobel Prize for polio virus cultivation, co-develops the first measles vaccine strain (Edmonston-B).
1963 – First measles vaccine licensed. Live attenuated vaccine developed by Enders et al. approved in the U.S. A live virus vaccine prepared in chick embryo tissue culture
1968 – Maurice Hilleman (1919–2005) American microbiologist. Developed the improved Edmonston-Enders strain (previously Moraten), which remains in use today as part of the MMR vaccine.
1989 – Two-dose MMR schedule introduced in U.S. Response to outbreaks in vaccinated children. Backed by ACIP, AAP, and AAFP.
2000 – Measles declared eliminated in the U.S. Defined as absence of continuous disease transmission for >12 months.
1998–2010 – Wakefield Hoax and Retraction. Andrew Wakefield publishes fraudulent paper linking MMR vaccine to autism (The Lancet, 1998). Paper retracted in 2010; Wakefield stripped of medical license.
2019–present – Resurgence linked to vaccine hesitancy. U.S. and global outbreaks intensify, particularly in undervaccinated populations despite >97% vaccine efficacy with two doses.
2023 – WHO reports over 107,000 measles deaths globally. Mainly among children under five; attributed to COVID-era immunisation gaps.
Associated Persons
- Francis Home (1719–1813). Demonstrated measles was caused by a blood-borne infectious agent.
- Peter Ludwig Panum (1820–1885). Documented measles transmission and lifelong immunity during the 1846 Faroe Islands epidemic
- Henry Koplik (1858–1927) – described Koplik spots useful for early detection of measles.
- Clement Dukes (1845-1925) – Introduced the numerical classification of childhood exanthems
- Thomas C. Peebles (1921–2010). Isolated the measles virus from a human host in 1954.
- John F. Enders (1897–1985). Co-developed the first licensed measles vaccine using the Edmonston strain.
References
Historical references
- Home F. Medical facts and experiments. 1759
- Panum PL. Observations made during the epidemic of measles on the Faroe Islands in the year 1846
- Enders JF, Peebles TC. Propagation in tissue cultures of cytopathogenic agents from patients with measles. Proc Soc Exp Biol Med. 1954 Jun;86(2):277-86.
Eponymous term review
- Enders JF, Peebles TC, McCarthy K, Milanovic M, Mitus A, Holloway A. Measles virus: a summary of experiments concerned with isolation, properties, and behavior. Am J Public Health Nations Health. 1957 Mar;47(3):275-82. doi: 10.2105/ajph.47.3.275.
- Enders JF. Vaccination against measles: Francis Home redivivus. Yale J Biol Med. 1961 Dec-1962 Feb;34(3-4):239-60.
- History of Measles. CDC
eponymictionary
the names behind the name
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |