
![]()
Funtabulously Frivolous Friday Five 272
Just when you thought your brain could unwind on a Friday, you realise that it would rather be challenged with some good old fashioned medical trivia FFFF, introducing the Funtabulously Frivolous Friday Five 272
Question 1
What is an Ogden fracture?
Reveal the funtabulous answer
Tibial Tubercle Fracture.
Ogden fractures occur most commonly amongst adolescent males near the end of the their skeletal growth. They are caused by the powerful contraction of the quadriceps creating an avulsion force on the tibial tubercle. They are more common in boys participating in sports such as football, basketball, high jump and running.

Classification of tibial tubercle fractures has undergone significant evolution. The original classification system was provided by Sir Reginald Watson-Jones which defined three types.
1955 Original classification by Sir Reginald Watson-Jones into Types I, II, III
- Type I: avulsion of small part of tibial tubercle, distal to the proximal tibial physis and without injury to the tibial epiphysis
- Type II: fracture extends across the physis but does not enter the knee joint. Epiphysis is lifted cephalad and incompletely fractured.
- Type III: avulsion which extended proximal to the physis into the knee. Displacement of the proximal base of the epiphysis with the fracture line extending into the joint
Original Watson-Jones classification (1955)

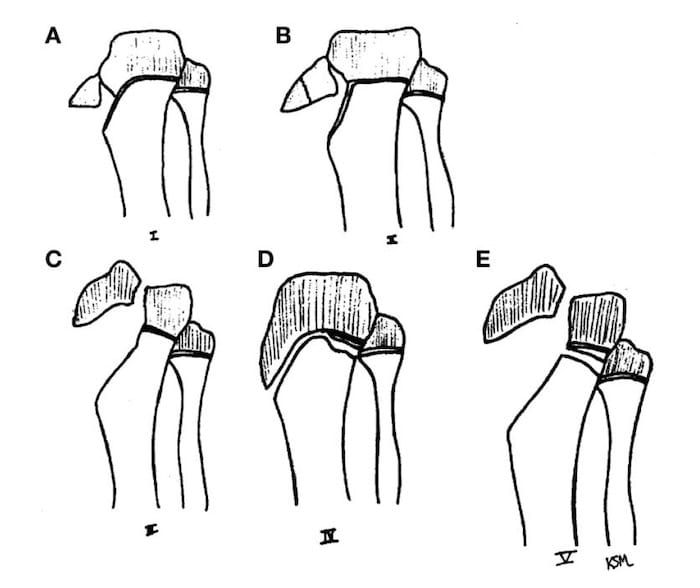
1980 Watson-Jones classification was modified by Ogden et al. to more accurately define specific fracture patterns and to establish treatment for different fracture types by including displacement and comminution. Classified into Types 1-3 [Modifier: A (nondisplaced), B (displaced)] [PMID 7358751]
Ogden tibial tubercle fracture classification (1980)

1985 Ryu and Debenham then suggested the addition of a Type IV which is a fracture of the tibial tuberosity that extends posteriorly along the proximal tibial physis creating an avulsion of the entire proximal epiphysis [PMID 3978913]
Ryu and Debenham Type IV tibial tubercle fracture (1985)
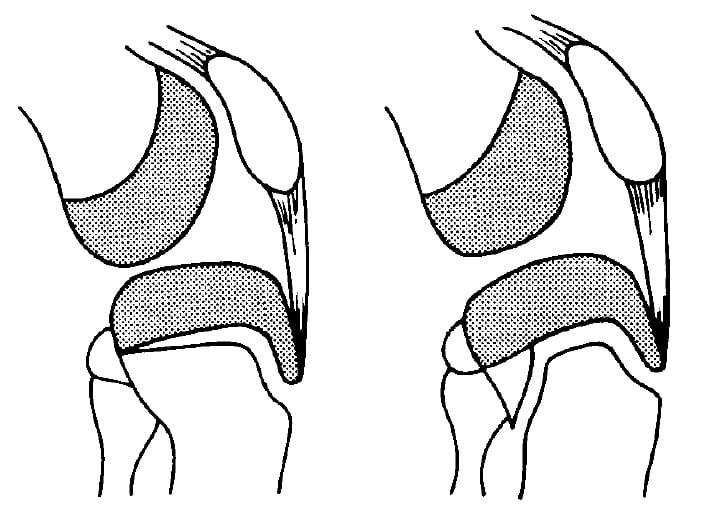
2003 McKoy and Stanitski proposed Type V which consists of a Type IIIB fracture with an associated Type IV fracture creating a ‘Y’ configuration. [PMID 12974489]
McKoy and Stanitski – Type V (2003)
References:
- Watson-Jones R. Injuries of the knee. In: Fractures and Joint Injuries. 1955; Vol. 2, Ed. 4 [Types I-III]
- Ogden JA, Tross RB, Murphy MJ. Fractures of the tibial tuberosity in adolescents. J Bone Joint Surg Am. 1980 Mar;62(2):205-15. [PMID 7358751] [Refined Types I-III with A and B modifiers ]
- Ryu RK, Debenham JO. An unusual avulsion fracture of the proximal tibial epiphysis. Case report and proposed addition to the Watson-Jones classification. Clin Orthop Relat Res. 1985 Apr;(194):181-4. [PMID 3978913] [Addition of Type IV ]
- Frankl U, Wasilewski SA, Healy WL. Avulsion fracture of the tibial tubercle with avulsion of the patellar ligament. Report of two cases. J Bone Joint Surg Am. 1990 Oct;72(9):1411-3. [PMID 2229123] [Addition of Type C modifier for fractures with associated patella ligament avulsion ]
- McKoy BE, Stanitski CL. Acute tibial tubercle avulsion fractures. Orthop Clin North Am. 2003 Jul;34(3):397-403. [PMID 12974489] [Addition of Type V ]
- Frey S, Hosalkar H, Cameron DB, Heath A, David Horn B, Ganley TJ. Tibial tuberosity fractures in adolescents. J Child Orthop. 2008 Dec;2(6):469-74. [PMC2656872]
Question 2
What triad signifies milk-alkali syndrome?
Reveal the funtabulous answer
Hypercalcaemia with metabolic alkalosis and renal insufficiency.
Milk-alkali syndrome is secondary to hypercalcaemia from an exogenous source (as opposed to hypercalcaemia from malignancy or hyperparathyroidism.
It is most commonly found in people who have an excess of calcium supplementation, either from over the counter preparations marketed for osteoporosis prevention, or equally in people who have seemingly over indulged in antacid preparations (heavy in aluminium hydroxide and magnesium carbonate).
Reference: Caruso JB et al. Health-Behaviour Induced Disease: Return of the Milk-Alkali Syndrome. J Gen Intern Med. 2007;22(7):1053-1055
Question 3
In a male patient presenting with his first cardiovascular event, what will approximately 2/3 of this population admit to experiencing for the first time in the preceding three years (usually only if directly asked)?
Reveal the funtabulous answer
Erectile dysfunction.
In male patients with co-existing erectile dysfunction and coronary artery disease, ED symptoms were reported as being clinically evident PRIOR to coronary symptoms in 67% of patients.
Men with known cardiovascular disease, hypertension and/or type II diabetes have an erectile dysfunction prevalence of 70%. The artery size hypothesis may help explain why patients with coronary artery disease do report erectile dysfunction before CAD is detected. This is because the lumen of the penile arteries is smaller that that of the coronary vessels, but are equally susceptible to the pathogensis of atherosclerotic disease and reduction of NO synthesis.
A penile artery has a lumen of 1-2mm, whereas the coronary artery lumen is usually 3-4mm; thus symptoms of impaired circulation in the penile arteries may be associated with sublinical plaque disease of other larger vessels.
So next time your are prescribing a dose of viagra perhaps have them swing by the chest pain clinic!
Reference: Montorsi F et al. Erectile dysfunction prevalence, time of onset and association with risk factors in 300 consecutive patients with acute chest pain and angiographically documented coronary artery disease. Our Urol. 2003;44(3):360-4
Question 4
Your redhead patient requires a hernia repair, they tell you the last time they needed anaesthesia they need extra amounts of anaesthetic because of their red hair. You’ve heard rumours that the red hair phenotype (and genetic ‘mutation’) may be associated with poorer sedative and anaesthetic outcomes, but is it true?
Reveal the funtabulous answer
No
Although some interesting original articles at the start of this century suggested that red heads (and their associated mutation in the melanocortin-1 receptor gene) had an increased anaesthetic requirement. A more recent publication in 2015 in the Canadian Journal of Anaesthesia seemingly put this rumour to bed.
A case-control cohort of n= 1,914 patients failed to demonstrate a differed between red heads and controls in to response to anaesthetic and analgesic agents or in recover parameters. Sorry, you get the same as everyone else in this regard.
Reference: Gradwohl SC et al. Intraoperative awareness risk, anaesthetic sensitivity, and anaesthetic management for patients with natural red hair: a matched cohort study. Can J Anaesth 2015;62(4):345-55
Question 5
The surgeon you refer your patient to groans when you mention your patient’s ginger phenotype stating “Rangas always bleed”. Do red haired patients bleed more?.
Reveal the funtabulous answer
No
One study attempted to show a link between red hair and bleeding after tonsillectomy (together with full moons and Friday the 13th). The incidence of post-tonsillectomy bleed was almost 7% but this was indistinguishable from that of the control group.
In another study, the bleeding tendencies between 50 women (half of whom had red hair and half black or brown hair) by using objective coagulation testing did not differ, despite the red haired women reporting significantly more subjective bruising in the perioperative period.
But could there still be another reason for the bleeding prejudice against redheads? Perhaps it is the inevitable association of red hair with ginger (of the Zingiber officinale variety). Ginger is commonly used as spice but is also used by herbalists to treat symptoms such as cough, abdominal pain, diarrhoea, nausea and motion sickness. Of greater relevance is that ginger can give people a tendency to bleed. Ginger may interact with the anticoagulant warfarin, inhibit platelet aggregation (by inhibition of thromboxane production from arachidonic acid) and increase fibrinolysis. So, it appears that ginger and bleeding are linked after all.
Reference:
- Cunningham AL et al. Red for danger: the effect of red hair in surgical practise. BMJ 2010;341:c6931
- LITFL – Are Redheads Bleeders?
…and finally
This prejudice against redheads is nearly as pervasive as that against lefties and no one expresses its impact better than our favourite Western Australian musico-comedic genius, Mr. Tim Minchin (includes colourful language of which your grandmother may disapprove)
…and equally importantly
- The author of this post is a redhead, and both his children are daywalkers
- One of the blog co-founders (before succumbing to an incantation of follicular expelliarmus…) was a ranga

FFFF
Funtabulously Frivolous Friday Five
Dr Mark Corden BSc, MBBS, FRACP. Paediatric Emergency Physician working in Northern Hospital, Melbourne. Loves medical history and trivia...and assumes everyone around him feels the same...| LinkedIn |