
![]()
Glyphosate toxicity
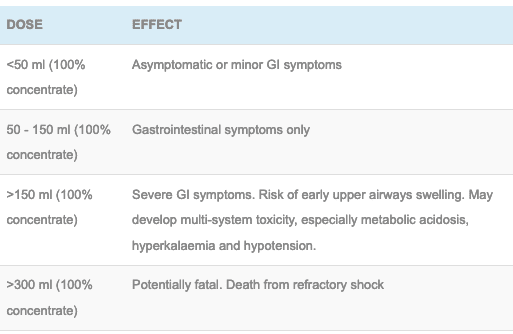
Glyphosate is a widely used herbicide. It can cause gastrointestinal corrosive symptoms and due to the surfactant that is present a severe metabolic acidosis, hyperkalaemia and cardiovascular collapse can occur.
Toxic Mechanism
The toxicity of glyphosate is largely due to the surfactant and other co-formulants. The mechanism is poorly understood but may involve disruption of cellular membranes and uncoupling of mitochondrial oxidative phosphorylation.
Toxicokinetics:
- Poorly but rapidly absorbed
- Peak concentration within 4 – 6 hours
- Not metabolised and eliminated in unchanged by the kidneys with a half life of 4 – 6 hours. This will be prolonged in those with renal impairment.
Resuscitation:
- Airway compromise: Intubate and ventilate especially if signs of oropharyngeal corrosive injury (stridor, dysphonia, throat pain, horseless or respiratory distress).
- Hypotension: Usually responds to fluid administration, noradrenaline is second line therapy [0.15mg/kg in 50ml D5W at 1-10ml/hr (0.05 – 0.5 mcg/kg/min)], other vasopressors may be used.
Risk Assessment
- The higher the concentration the greater the risk, most solutions are diluted and these will result in minor gastrointestinal irritation.
- Cutaneous exposures can cause minor irritation but not systemic toxicity.
- Acute corrosive injury to the upper airway poses an immediate life threat.
- Poor signs are: tachycardia, abnormal chest x-ray, metabolic acidosis, hyperkalaemia, acute renal impairment, liver impairment and older age.
- Children: minor ingestions do not need assessment unless symptoms develop.
- Clinical features:
- Involve the expected symptoms from GI irritation: Nausea, vomiting, diarrhoea and abdominal pain.
- Respiratory from upper respiratory tract irritation (cough) with the potential for aspiration pneumonititis and rare case of non-cariogenic pulmonary oedema.
- In severe cases hypotension and cardiovascular collapse can occur.
Supportive Care
- Analgesia and antiemetics.
Investigations
- Screening: 12 lead ECG, BSL, Paracetamol level
- Specific:
- Glyphosate levels are not readily available or clinically useful
- EUC and LFTs to detect dysfunction or hyperkalaemia
- Acid-base balance and lactate to detect acidosis
- Chest x-ray to evaluate for aspiration pneumonitis or pulmonary oedema
- Endoscopy/CT chest: Not usually indicated as severe corrosion would be unusual
Decontamination:
- Not indicated and technically difficult due to vomiting.
Enhanced Elimination
- Haemodialysis will eliminate glyphosate but is generally not indicated unless there is severe acidosis and acute renal injury.
Antidote
- None available.
Disposition
- Patients who are clinically well at 4 hours can be medical cleared. Discharge should not occur at night.
- If patients are symptomatic they will require close monitoring in an HDU environment to detect any signs of early cardiovascular collapse. Also any patient who has ingested >150 ml of 100% glyphosate requires HDU/ICU as multiple organ effects will be expected to occur within 24 hours.
Additional Resources and References:
Additional Resources:
- CCC – Corrosive ingestion
References:
- Bradberry SM, Proudfoot AT, Vale JA. Glyphosate poisoning. Toxicological Reviews 2004; 23(3):159-167.
- Chen H-H, Lin J-L, Huang W-H et al. Spectrum of corrosive oesophageal injury after intentional paraquat or glyphosate-surfactant herbicide ingestion. International Journal of General Medicine 2013; 6:677-683
- Lee CH, et al. The early prognostic factors of glyphosate-surfactant intoxication. American Journal of Emergency Medicine 2008; 26:275-281.
- Lee HL, Chen KW, Chi CH et al. Clinical presentations and prognostic factors of glyphosate-surfactant herbicide intoxication: a review of 131 cases. Academic Emergency Medicine 2000; 7(8): 906-910.
- Roberts DM, Buckley NA, Mohamed F et al. A prospective observational study of the clinical toxicology of glyphosate-containing herbicides in adults with acute self-poisoning. Clinical Toxicology 2010; 48:129-136

Toxicology Library
DRUGS and TOXICANTS
Dr Neil Long BMBS FACEM FRCEM FRCPC. Emergency Physician at Kelowna hospital, British Columbia. Loves the misery of alpine climbing and working in austere environments (namely tertiary trauma centres). Supporter of FOAMed, lifelong education and trying to find that elusive peak performance.

Hi J,
I think that question is beyond the scope of this article and our expertise.
However, from my very limited knowledge; there was a recent systematic review (2022) looking at chronic exposure and the potential for neurological changes (looks like it was based on rat studies, though). As someone who also has a lifelong exposure to glyphosate — it is certainly something of interest to me. My general understanding is that glyphosate (fortunately) seems to be one of the less harmful synthetic herbicides widely used, and seems to have been one of the most studied agent due to ongoing concerns of human exposure, with limited evidence of significant harm despite massive doses (like, 100s of milligrams per day orally) of continuous exposure (again based on animal studies). I’m very happy for my lack of understanding to be rapidly corrected by anyone with substantial knowledge in the field!
Good luck in your quest for further information and understanding.
James