![]()
Henry Janeway
Henry Harrington Janeway (1873-1921) was an American physician and pioneer for radiation therapy in the treatment of cancer.
Janeway was the first to design a laryngoscope specifically for anaesthesia and introduced the novel feature of a battery powered laryngoscope. His interest in anaesthesia extended to mechanical ventilation where his experiments in dogs with colleague Dr Nathan Green, lead to the development of the ‘rhythmic inflation apparatus’ – an intermittent positive pressure ventilator. Whilst it never entered clinical practice, it was a forerunner for modern ventilators that followed.
Janeway and Green also collaborated to develop the ‘Green button’ a technique for gastric anastomosis after resection of cardial gastric carcinoma. His work in gastroenterology saw him introduce the Janeway gastrostomy procedure, a technique which stands the test of time and is still used in palliative care medicine today.
Janeway is most credited for his pioneer work in radiation therapy and was the first to advance the use of radium as a first line therapeutic agent in cervical carcinoma. His technique for burying radium emanation into the cervix, the use of dental modelling compound to enhance the application of radium and the use of radium emanation needles, all originated from his clinic.
Janeway lead a short but illustrious career with multiple contributions to the fields of anaesthesia, gastroenterology, surgery and radiation oncology; ironically it was the cancer he so intensely researched and sought to treat that took his own life. The Annual Janeway Lecture and Medal, stands to honour this distinguished man.
Biography
- Born on March 19, 1873 in New Brunswick, New Jersey
- 1889 – Graduates from Rutgers College
- 1898 – MD, College of Physicians and Surgeons
- 1898-1900 Internship at Roosevelt Hospital
- 1906 – Commences work in the experimental laboratories of his medical school and specialises in surgery and dermatology
- 1907 – Dermatological practice with his father-in-law Dr Bulkley for the next two years and publishes several articles about skin and cancer pathology
- 1909 – Chief of the Laboratory for Experimental Research of Physicians and Surgeons and conducts work in gastric and oesophageal surgery, blood pressure and shock; collaborates with Dr Nathan W Green and develops the ‘Green button’ for surgical anastomosis of the oesophagus and stomach; published in JAMA with step-by-step guide ‘Experimental intrathoracic esophageal surgery’
- 1910 – Collaborates again with Green in experimenting with mechanical ventilation during thoracic surgery on animals; publishes findings in Annals of Surgery as “Artificial respiration and intrathoracic oesophageal surgery.’; devises an apparatus coined ‘rhythmic inflation apparatus’ to deliver positive pressure ventilation.
- 1913 – Publishes article on Intra‐tracheal anesthesia from the standpoint of the nose, throat and oral surgeon with a description of a new instrument for catheterizing the trachea and devises a new laryngoscope to include a battery powered light source, the first of its kind.
- Proposes a novel method for gastrostomy, described in his paper on ‘The relation of gastrostomy to inoperable carcinoma of the esophagus: with a description of a new method of performing gastrostomy’ – and so the term ‘Janeway Gastrostomy’ is coined
- 1914 – Attending Surgeon and Chief of the Radium Department at Memorial Hospital in New York where he develops and advances the use of radium as a therapeutic agent in cancer; Janeway is the first to advocate for radium use in the treatment of cervical cancer by ‘burying radium emanation’ in the cervix.
- 1917 – Publishes multiple articles on Radium therapy in cancer including his landmark article on ‘The Treatment of Uterine Carcinoma’
- Dies on February 1, 1921, aged 47 from cancer
Medical Eponyms and Key Medical Contributions
Janeway Laryngoscope (1913)
Janeway was the first anaesthetist to publish an article on direct laryngoscopy; prior articles about laryngoscopy were within the domain of surgeons. His landmark paper ‘intratracheal anaesthesia from the standpoint of the nose, throat and oral surgeon with a description of a new instrument for catheterising the trachea’ introduced the novel design of a battery powered laryngoscope, the first of its kind specifically designed for anaesthesia. Initial designs were complex and included a telescopic prism with eye piece to visualise the catheter and larynx. A central notch kept the catheter midline during placement
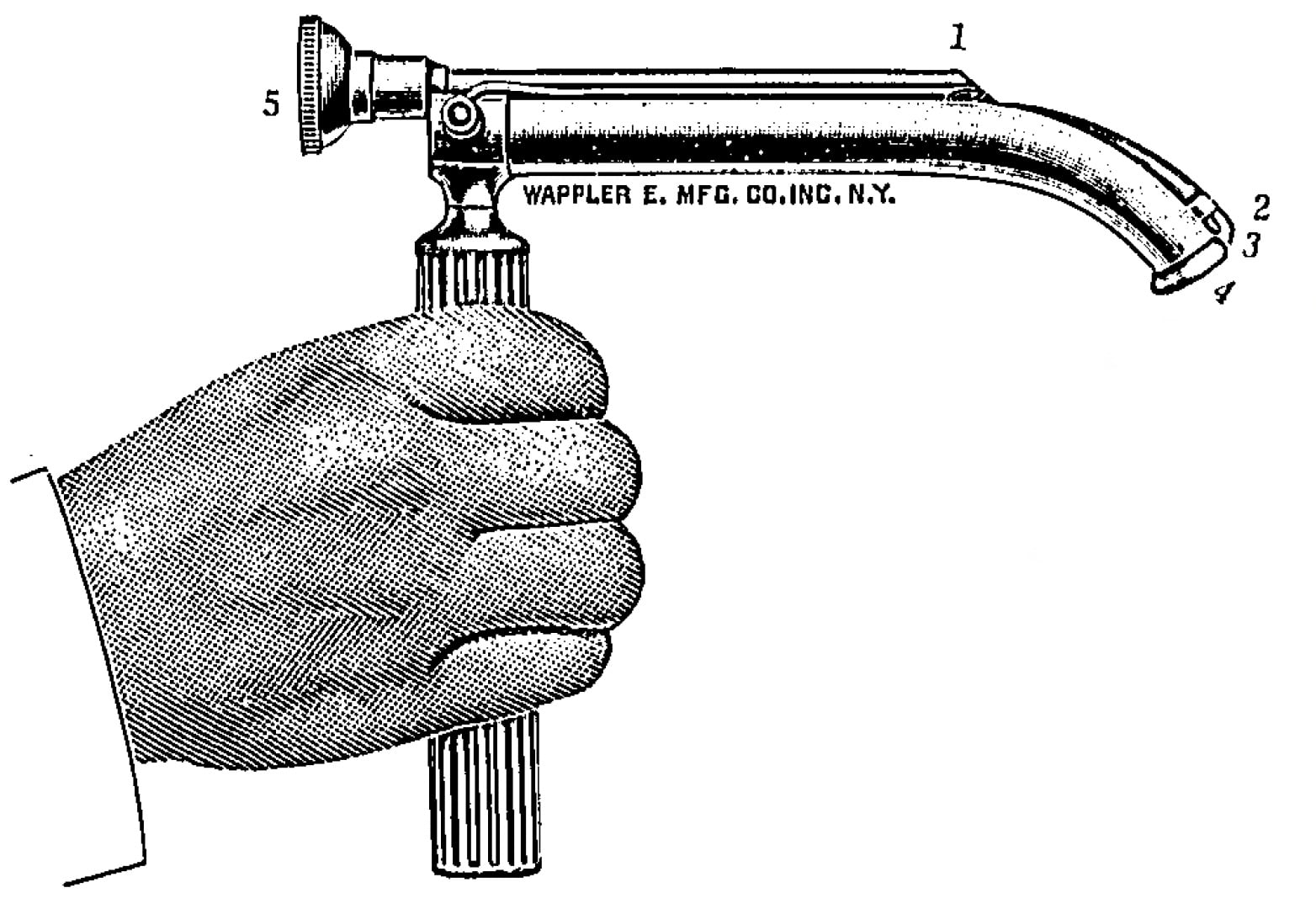
1. Prism. 2. Lamp. 5. Objective glass through which the eye of the observer views the larynx in the direction of 3-4
He later improved on this to include a distal light source with the battery incorporated within the handle of the laryngoscope itself and a blade that was shortened and curved at its distal end to facilitate delivery of the catheter through the vocal cords. Because catheter placement could now occur under direct vision, it obliviated the need for the complex prism mechanism.
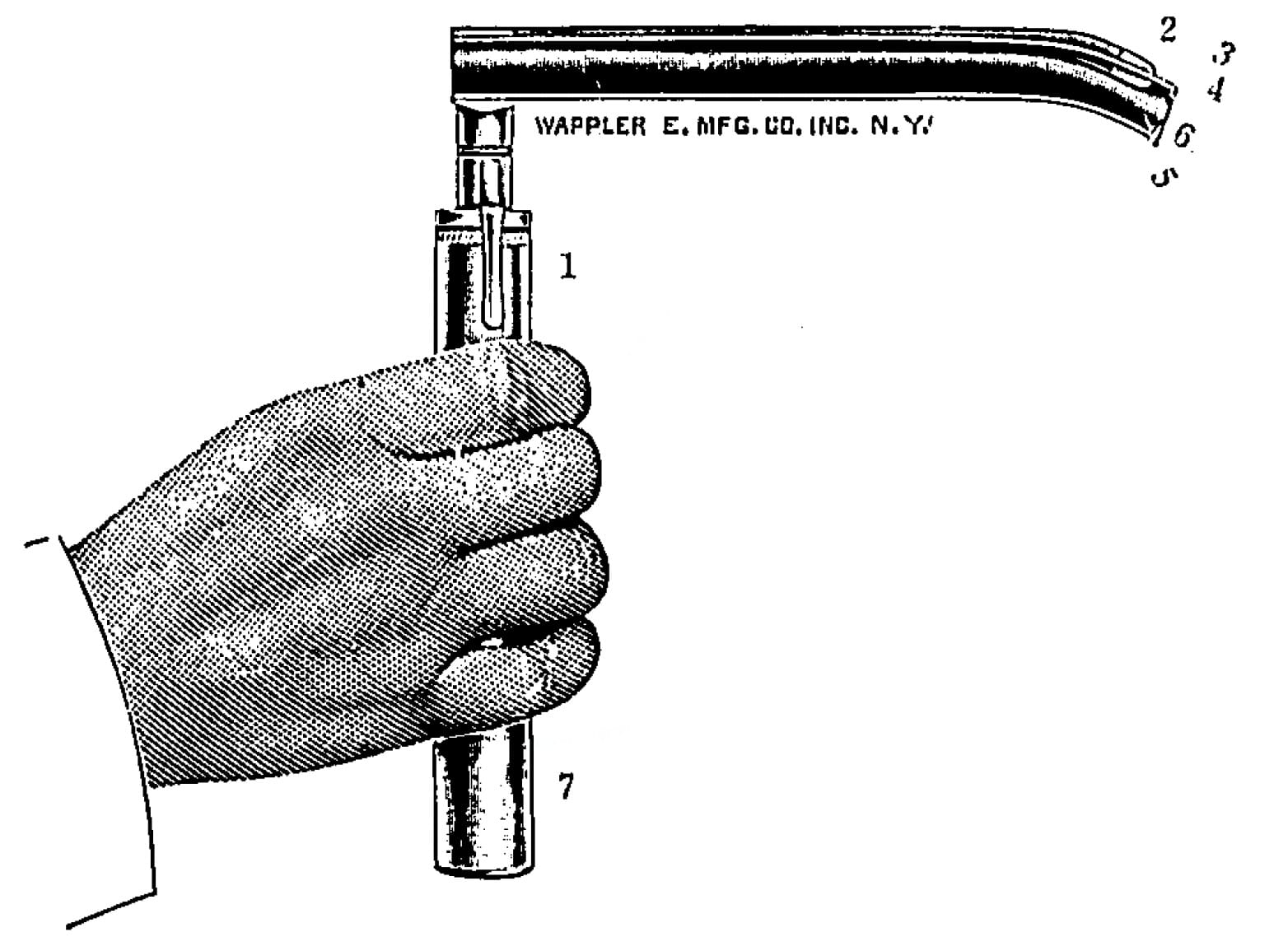
1. Press button for illuminating the lamp. 2. Lamp. 3-4 Direction of vision. 5-6. Direction taken by the catheter. 7. Handle containing two dry cells
Of his invention, he remarks:
…offers a very great advantage. It permits of easy catheterization of the larynx even when the patients’ pharyngeal reflexes are not completely abolished and without the necessity for the same degree of extension of the head. The omission of the telescope greatly simplifies the instrument
Laryngoscope. 1913
Whilst Janeway experienced much success with his invention in head and neck and thoracic procedures, his laryngoscope never gained widespread popularity
Gastric surgery
The risk of infection when the oesophagus was opened operatively was a well recognised issue at the time. Janeway’s experimental work in thoracic surgery in animals was met with disaster
Not one case of carcinoma of the cardia operated upon the transthoracic route has been reported that has lived more than five days…in looking over the results of this last winter’s work…we have operated upon over 50 animals…the animals die with pus in the chest, with collapsed lungs, often with a general infection, or with exhaustion from labored breathing…
Where and from what does the infection come? To a certain extent by direct contamination from the opened viscera”
New York Surgical Society. 1911
His collaboration with Dr Nathan Green resulted in the development of the ‘Green button’ which allowed anastomosis between the oesophagus and stomach without freely opening either organ.
By the pressing together of the opposing halves of the button through the approximated and unopened walls of the oesophagus and stomach a union of these viscera is effected without the slightest contamination of the field of operation, and more rapidly than it can be done by any other method
Green NW, Janeway HH, Ann Surg 1910
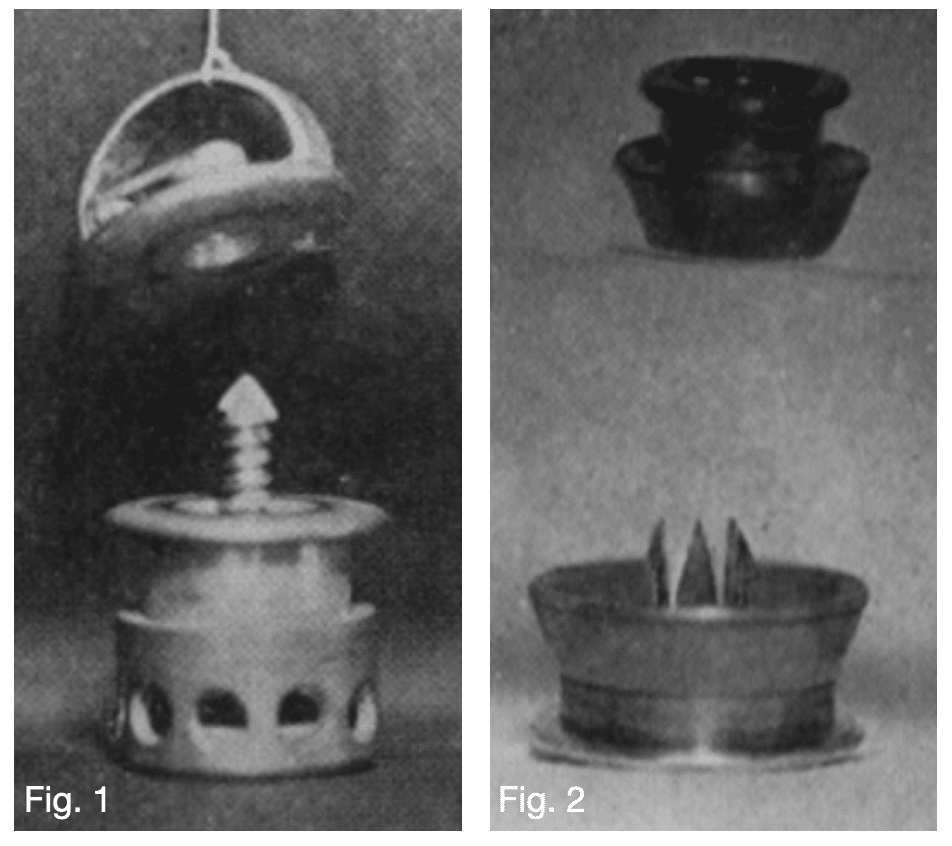
Fig 2: Button for end-to-side anastomosis.
Green NW, Janeway HH, Ann Surg 1910
Janeway Gastrostomy (1913)
Janeway’s interest in gastroenterology and intrathoracic surgery lead him to develop a method for performing a gastrostomy which endures today in the nomenclature as ‘Janeway gastrostomy.’
A tunnel is created from the anterior wall of the stomach which is brought to the skin to form a permanent stoma. A small-bore tube can then be later introduced into the opening to deliver medications and or food.
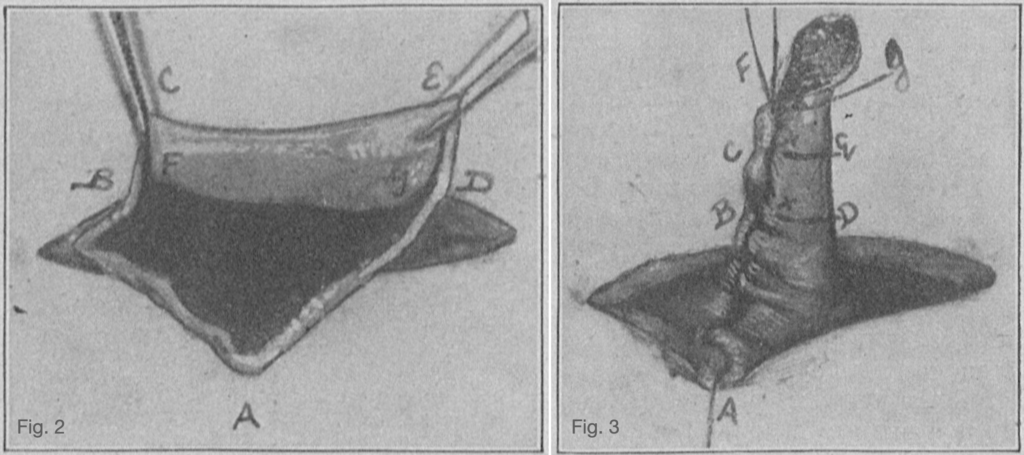
Fig 3: New canal, tubular in shape, formed by after-suture of plastic procedure shown in Fig 2.
Janeway HH, JAMA. 1913
The standard procedure today is percutaneous endoscopic gastrostomy however the Janeway gastrostomy still maintains relevance and is used for palliative feeding access or in patients where PEG is impractical.
Radiation therapy
Radiation therapy was first used in the treatment of cancer by Willian B. Colley (1862-1936) in 1903 who described 84 patients with tongue cancer treated with radiation therapy alone. Unfortunately, because of poor results Colley was unsuccessful in purporting radiation therapy as treatment in cancer and it fell off the medical radar for 8 years.
Enter Janeway and radiation therapy as a treatment modality for cancer is reintroduced with his landmark paper ‘The Treatment of Uterine Carcinoma by Radium’ in 1919 considered a classic in radiation oncology history.
Janeway developed a technique of burying radium emanation in the cervix. He used dental modelling compound to improve radium delivery to the carcinoma site. A mould of the tumour is taken and the lesion of interest is marked on the mould with ink. Grooves are then made with a hot tool and radium tubes placed within these grooves which are then filled with paraffin. This method ensured that radiation is delivered to the target area and remained in position throughout the duration of treatment.
Janeway strongly advocated for radium treatment for local or borderline resectable cancers and argued for radical abdominal surgery in cases of lymphatic metastases. This duality in treatment strategies – i.e. radiation for primary lesions and surgery for regional lymph node metastasis – became the central concept of cancer management. About radiation treatment, Janeway remarked:
The characteristic of the result among cases cured by radium coupled with the ease by which this result can be obtained far surpasses the results of surgical ablation
Am J Roentgenology. 1918
Of historical significance
Janeway developed a lump on his jaw shortly after graduating medical school. It was proved to be cancerous and Janeway underwent multiple surgeries throughout his life in attempt to cure the cancer that would eventually take his life.
The dissatisfaction with the then current methods for treatment, lead him to pursue his research into radium as a therapeutic agent. It is of great misfortune, that his successes as a physician could not be used to save his own life, however if not for this twist of fate, the many patients who followed may not have benefited from his work.
Janeway Medal and Janeway Lecture
Since 1933, the American Radium Society has sponsored an annual lecture in memory of Janeway and his pioneering work in the therapeutic use of radium.
Lecturers are chosen on the basis of their outstanding scientific contributions. Each lecturer is presented the handsome Janeway Medal. The Medal was originally a large bronze medal, but was changed to a gold medal in 1971.
The first ever Janeway Memorial Lecture was given by his friend Dr James Ewing entitled: Early experience in Radiation therapy [American journal of roentgenology, 1934; 31: 153-190]
Mechanical ventilation
Green and Janeway rhythmic inflation apparatus (1910)
The ability to maintain adequate respiration during thoracic procedures on the open chest was a surgical conundrum during that time. Janeway and Green conducted myriad animal experiments in an effort to circumnavigate this problem.
During their experiments, it was observed that thoracic surgery was more successful when performed under mechanical ventilation
…in working with the intralaryngeal cannula it was noticed that the alternating increase and decrease in intratracheal pressure produced an artificial apnoea which largely eliminated the movements of the diaphragm. The advantages of such an elimination of movement during operation were so apparent that it induced the other of use…to devise another cabinet provided with a mechanism with accomplished during operation a similar cessation of respiratory movements
Green and Janeway. Ann Surg 1910
This lead Janeway and Green to devise a ventilator based on Brauer’s invention for application of intermittent positive pressure ventilation.
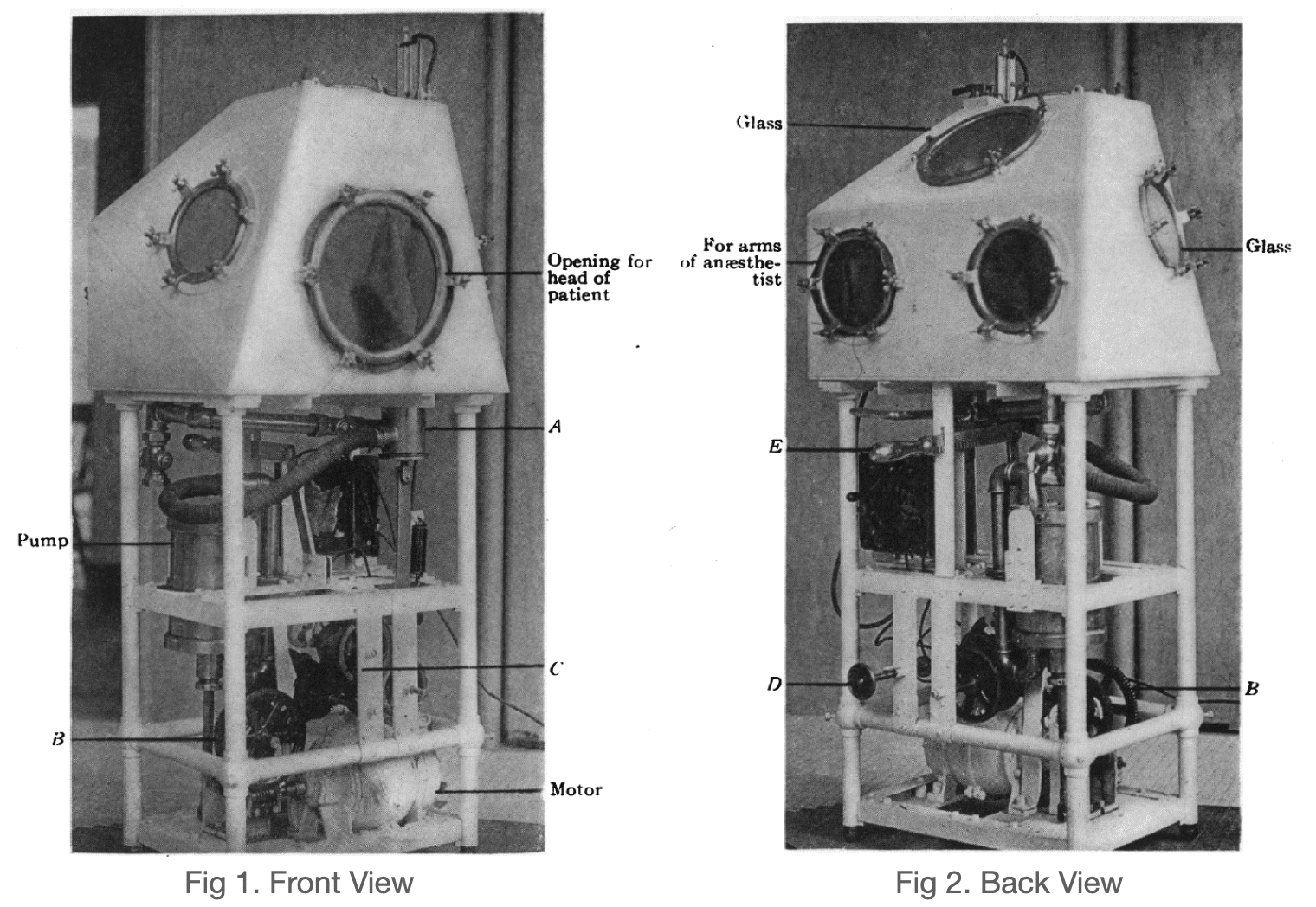
The apparatus consisted of a box with an opening for the patients’ head and for the anaesthetists’ arms to access the patient ‘in case of vomiting or the necessity of cleaning out the pharynx or passing an instrument into the oesophagus or stomach‘
A pump and motor were positioned under the box and a valve (A) controlled by gears (B) and a cone shaped cam (C) allowed intermittent pressure ventilation to be delivered within the cabinet. Respiration rate and inspiratory-expiratory ratio could be adjusted by the anaesthetist by use of a lever (D and E respectively)
Respiration may be uninterruptedly continued with use of such an apparatus….by this apparatus we have kept a fully curarized dog alive for four hours
Green and Janeway. Ann Surg 1910
It was also remarked that because of ‘cerebral anaemia’ induced by the positive pressure surrounding the patients’ head, a lesser amount of ether was required to induce anaesthesia.
While the ‘rhythmic inflation’ apparatus of Janeway and Green was successful in experimental conditions, it never found a place in clinical practice.
Major Publications
- Green NW, Janeway HH. Experimental intrathoracic esophageal surgery. JAMA. 1909; LIII(24): 1975-1978 [Green button]
- Green NW, Janeway HH. VI. Artificial Respiration and Intrathoracic Oesophageal Surgery. Ann Surg. 1910; 52(1): 58-66.
- Janeway HH, Green NW. VII. Cancer of the OEsophagus and Cardia: A Description of an Operation for its Removal by the Transthoracic Route Under Conditions of Differential Pressure. Ann Surg. 1910; 52(1): 67-82
- Green NW, Janeway HH. IX. An Experimental Study of the Management of Post-Operative Thoracic Infections: A Preliminary Report. Ann Surg. 1911; 54(4): 549-53
- Janeway HH, Green NW. Esophagoscopy and gastroscopy. Surgery, Gynecology & Obstetrics. 1911; 13(3): 245-253
- Janeway HH. IX. An Apparatus for Intratracheal Insufflation. Ann Surg. 1912; 56(2): 328-30.
- Janeway HH. Intra‐tracheal anesthesia from the standpoint of the nose, throat and oral surgeon with a description of a new instrument for catheterizing the trachea. The Laryngoscope. 1913; 23(11): 1082-1090 [Janeway Laryngoscope]
- Janeway HH. The relation of gastrostomy to inoperable carcinoma of the esophagus: with a description of a new method of performing gastrostomy. JAMA. 1913; 61(2): 93-95 [Janeway gastrostomy]
- Janeway HH. Results of radium in cancer. JAMA. 1914; LXII(22): 1707-1709
- Janeway HH. XIV. Simple and Complete Forms of Apparatus for Intratracheal Anaesthesia. Ann Surg. 1914; 59(4): 628-30
- Janeway HH. The Nervous System; The Special Senses; The Circulation; Digestion; Hygiene;
- The kidney and bladder; The ductless glands. Lecture notes on physiology. 1915
- Janeway HH. Radium therapy in cancer at the Memorial Hospital, New York (First report: 1915-1916). New York, P. B. Hoeber, inc 1917
- Janeway HH. Cancer of the mucous membranes treated with radium alone. The American Journal of Roentgenology. 1918; 5: 414-421.
- Janeway HH. The treatment of tumors of the superior maxilla. Ann Surg. 1918; 68(4): 353-70
- Janeway HH. The Treatment of Cancer of the Lip by Radium: A Report of Twenty-four Cases. Journal of the American Medical Association, 1918; 70(15): 1051-1058.
- Janeway HH. The Treatment of Uterine Carcinoma by Radium. Surgery, Gynecology & Obstetrics. 1919; 29: 242-265
- Janeway HH. The treatment of malignant tumors of the thymus gland by radium. Ann Surg. 1920 Apr;71(4):460-71
- Janeway HH. Treatment of cancer, particularly of the tongue, tonsil and rectum, by buried emanation,
- The American Journal of Roentgenology. 1920; 7: 92-101
- Janeway HH. Radium therapy in cancer at the Memorial Hospital, New York (Second report). New York, P. B. Hoeber, inc 1923
References
Biography
- Obituary. Dr Henry H. Janeway. Radium. 1921; 16(6): 81-82
- Henry Harrington Janeway. In: 50th Anniversary Book, The American Association for Thoracic Surgery (AATS)
- Bibliography. Janeway, Henry Harrington 1873-1921. WorldCat Identities
Eponymous terms
- Edling L. On Plastic Means of Application in Radium Therapy, Acta Radiologica, 1921;1(1):60-88
- Fletcher GH. Cancer of the uterine cervix. Janeway lecture, 1970. Am J Roentgenol Radium Ther Nucl Med. 1971 Feb;111(2):225-42.
- Minard G. The history of surgically placed feeding tubes. Nutr Clin Pract. 2006 Dec;21(6):626-33.
Eponym
the person behind the name

FACEM. Emergency physician and researcher at Sir Charles Gairdner Hospital, Perth
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |