
![]()
Hypernatraemia and Acidosis
aka Metabolic Muddle 005
A 20 year old male presents with 3 days of lethargy and generalised malaise. He is confused and looks very unwell.
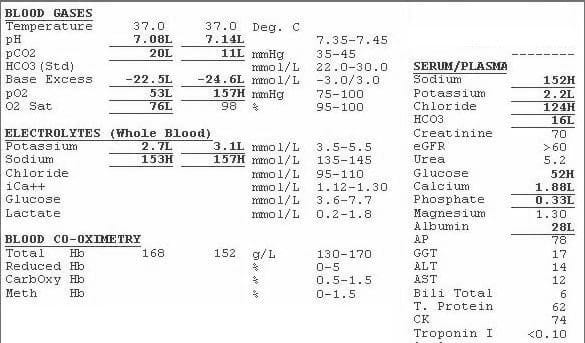
The following blood tests are obtained:
Questions
Q1. Describe the acid base disturbance.
Answer and interpretation
There is a severe metabolic acidosis with a raised anion gap with an appropriate degree of respiratory compensation.
Q2. What is the likely diagnosis?
Answer and interpretation
Diabetic ketoacidosis
Q3. Describe the electrolyte abnormalities.
Answer and interpretation
The patient has hypernatraemia and, in fact, is even more hypernatraemic than is immediately apparent. The glucose is very high and, therefore, a correction is required.
The calculation is:
[Na+] + (glucose -10)/3
In other words, the corrected sodium is 166.
The potassium is very low. This is particularly noteworthy given the degree of acidaemia. Acidaemia drives the potassium up so, as the acid base disturbance is corrected, the potassium will drop even further. While total potassium deficits can be difficult to predict on the basis of serum potassium, the total loss here is likely to be in the order of 100s mmols.
The magnesium is not low which would be unheard of in this setting unless the patient had received magnesium supplementation (which they had).
The phosphate is low – this too is a common electrolyte disturbance in DKA. There is debate about the significance of low phosphate in this setting but Intensivists (myself included) can’t resist correcting the phosphate.
Q4.Should the corrected sodium be used for calculating the anion gap?
Answer and interpretation
No!
The anion gap reflects the balance between positively and negatively charged electrolytes in the extracellular fluid. Glucose is electrically neutral and does not directly alter the anion gap. However, glucose is osmotically active so water is pulled into the extracellular fluid. This has a dilutional effect on all extracellular electrolyte concentrations, both positive or negative, and so the anion gap is minimally altered.
Q5. It emerges that the patient has recently been diagnosis with Schizophrenia and has commenced olanzapine. What is the significance of this additional history?
Answer and interpretation
There are some data that suggest an increased risk of diabetes and diabetic ketoacidosis in patients commenced on atypical antipsychotics.
Q6. An amylase is measured and is found to be 3 times the upper limit of normal. What is the significance of this finding?
Answer and interpretation
Mild elevations in amylase are common in diabetic ketoacidosis and in the absence of other manifestations suggestive of pancreatitis are not of clinical significance.
References
- Beck LH. Should the actual or the corrected serum sodium be used to calculate the anion gap in diabetic ketoacidosis? Cleve Clin J Med. 2001 Aug;68(8):673-4. [PMID 11510523]
CLINICAL CASES
Metabolic Muddle
Intensivist in Wellington, New Zealand. Started out in ED, but now feels physically ill whenever he steps foot on the front line. Clinical researcher, kite-surfer | @DogICUma |
Why is the chloride so high? Surely, there is a significant element of NAGMA here too?
Met Acidosis, NAGMA (AG = 152-124-16 = 12).
…but Albumin is 28… Low albumin (a negative anion) artificially lowers the anion gap.
AGCorr = AG + (42-28)/4 = 12 + 3.5 = 15.5