
![]()
Is resistance futile?
aka Pulmonary Puzzler 011
A 79 year-old male presents with fevers and worsening respiratory distress. He has a past history of a right-sided lobectomy for lung cancer.
The following chest X-ray is obtained:

Questions
Q1. Describe the chest X-ray.
Answer and interpretation
There is extensive air space change involving the right middle and lower zones and the left lower zone. There is loss of volume in the right side of the chest consistent with previous surgery. Given the history, the findings are suggestive of severe pneumonia.
The following arterial blood gas is obtained:
Arterial Blood Gas
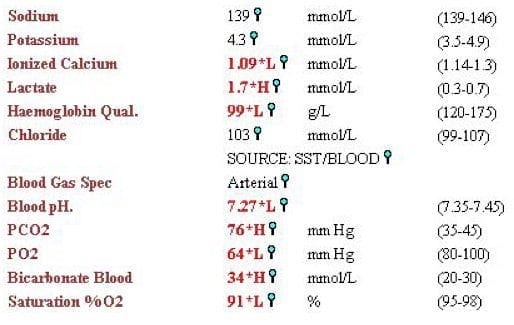
Q2. Describe the arterial blood gas.
Answer and interpretation
The oxygen saturation and the PaO2 are low. The patient is acidaemic and there is a respiratory acidosis.
The expected HCO3 if this was an acute disorder would be approximately 30 (HCO3 increases by 1 for every 10mmHg increase in CO2 for an acute disorder). However, the actual bicarbonate is higher than this. If the change in CO2 was all chronic the expected HCO3 would increase by 4 for every 10mmHg increase in CO2 i.e. a bicarbonate of approximately 40 would be expected. The bicarbonate is actually about half way between these two predicted values.
This is consistent with acute-on-chronic type 2 respiratory failure.
The patient is intubated for worsening respiratory failure. Among other investigations, a urinary pneumococcal antigen is performed which is positive. The patient is treated with penicillin. A few days later the following chest X-ray is obtained.

Q3. Describe the chest X-ray.
Answer and interpretation
- The patient is intubated and lined.
- The consolidation is worse.
The bronchial washing specimen confirms Streptococcus pneumoniae which is RESISTANT to Penicillin
Q4. Is penicillin an appropriate choice to treat this infection?
Answer and interpretation
This is a complicated question.
The serum concentrations of penicillin that can be achieved with intravenous therapy are greater than the MIC even for highly resistant pneumococci and penicillin penetrates lung tissue very well (this is not the case for meningitis where relatively poor CNS penetration may limit the effectiveness of penicillin).
In a prospective study of children with community acquired pneumococcal infections due to pneumococcus treated with penicillin, there was no difference in mortality based on whether pneumococci were penicillin-resistant or penicillin-sensitive. However, in this and other studies, the number of patients with an MIC of >4mcg/ml is very small. It is not known whether highly active beta lactams such as ceftriaxone are more rapidly efficacious than penicillin for highly resistant strains — this simply has not been studied.
The key issues are probably dose and MIC.
Giachetto et al (2004) reported adequate interdose time serum concentrations of greater than 4mcg/ml using 200 000 units/kg/day. So, in summary if the MIC is 2mcg/ml or less there are prospective data that suggest that standard dose penicillin is just fine. If the MIC is more than 2mcg/ml there are no prospective data that support use of penicillin; however, provided that a high dose of penicillin is used, penicillin is likely to be effective — although, using an alternative beta lactam is this setting would be reasonable.
Q5. How should wounds such as this be appropriately explored?
Answer and interpretation
Q6.
Answer and interpretation
Q6.
Answer and interpretation
Q6.
Answer and interpretation
Q6.
Answer and interpretation
Q6.
Answer and interpretation
Q6.
Answer and interpretation
Q6.
Answer and interpretation
Q6.
Answer and interpretation
Q6.
Answer and interpretation
References
- For more Pulmonary cases check out the LITFL Top 150 Chest X-Rays
- Cardoso MR, Nascimento-Carvalho CM, Ferrero F, et al. Penicillin-resistant pneumococcus and risk of treatment failure in pneumonia. Arch Dis Child. 2008 Mar;93(3):221-5. Epub 2007 Sep 11. PMID: 17848490.
- Clifford V, Tebruegge M, Vandeleur M, Curtis N. Can pneumonia caused by penicillin-resistant Streptococcus pneumoniae be treated with penicillin? Best Bets 11 Feb 2010
- Giachetto G, Pirez MC, Nanni L, et al . Ampicillin and penicillin concentration in serum and pleural fluid of hospitalized children with community-acquired pneumonia. Pediatr Infect Dis J 2004;23:625–9. PMID: 15247600

CLINICAL CASES
Pulmonary Puzzler
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |