
![]()
John Hughlings Jackson
John Hughlings Jackson (1835-1911) was an English neurologist.
Jackson was a giant of neurology. He studied epilepsy, aphasia, apraxia, stroke, and functional localisation to define levels of organisation within the nervous system which laid the foundations of modern neurology.
He defined the nature of the relationship between mind and brain, and psychophysical parallelism—mental states arose during but not from the activities of the brain; movements and their organisation; speech and loss of speech; the duality of symptoms, positive and negative; the hierarchy of levels in the nervous system; and the evolution and dissolution in the nervous system [Walshe, 1961]
Jackson was recognised in the field of ophthalmology for promoting the importance of the use of the ophthalmoscope; the nature of optic neuritis and atrophy; headache as a result of refractive errors; ocular vertigo; and the anatomical innervation of levator palpebrae superioris by the fifth as well as the third cranial nerve in the Marcus Gunn syndrome. [Taylor, 1915]
Contributions in the area of speech include the differentiation between speechlessness and plentiful words wrongly used; between internal and external speech; and between intellectual and propositional speech. He noted that the loss of power of performance varies with the complexity of the act; recognised the power of intellectual expression by movements of any kind; and the characterisation of agnosia as non-language aphasia. [Head, 1915]
Biography
- Born April 4, 1835 Providence, Yorkshire
- apprenticed to a physician in York, training further at St. Bartholomew’s Hospital in London before working in a Poor-Hospital in York and then at the London Hospital and Moorfields Eye Hospital
- 1862 – assistant physician to the National Hospital, a position secured with the assistance of Charles Brown-Sequard (1817-1894)
- 1863 – staff physician, London Hospital
- 1878 – Fellow of the Royal Society; founded the journal Brain founded in 1878 along with Sir John Charles Bucknill (1817-1897), David Ferrier (1843-1928) and James Crichton-Browne (1840-1938)
- 1894 – retired from practice at the London Hospital
- 1906 – retired from practice at the National Hospital
- Died October 7, 1911, London
Medical Eponyms
Jacksonian march [Jacksonian epilepsy, Bravais-Jackson epilepsy]
The spread of tonic-clonic epileptic movements through contiguous body parts on one side of the body as the causative epileptic discharge successively excites adjacent cortical regions
Early description provided by Louis François Bravais (1801–1843) in his thesis of 1827 ‘Recherches sur les symptômes et le traitement de l’épilepsie hémiplégique‘. Bravais described 25 cases of what he termed “hemiplegic epilepsy”. These cases featured unilateral convulsions and postictal hemiparesis. Bravais focused strictly on descriptive phenomenology and did not infer mechanisms. Charcot termed the seizures Épilepsie Bravais-Jacksonienn in 1877
Robert Bentley Todd (1809-1860) in his Lumleian lectures (1849) described the association of local contralateral cerebral surface pathology with unilateral convulsing. Todd described a temporary paralytic state that sometimes remained after epileptic convulsions, particularly when the convulsions had affected only one side of the body or one limb (Todd’s palsy). He called these unilateral convulsions with paralysis ‘epileptiform’
A paralytic state remains sometimes after the epileptic convulsion. This is more particularly the case when the convulsion has affected only one side or one limb: that limb or limbs will remain paralytic for some hours, or even days, after the cessation of the paroxysm, but it will ultimately perfectly recover.
In 1863, Jackson reported the seizure activity of a 33-year old female suffering ‘attacks of convulsion of the left arm and left side of the face‘.
…one day whilst at tea, she felt a glimmering over the eyes, then ” it took the elbow, next the hand, so that all the fingers worked together,” and het face was drawn to the left side. She then became insensible. She did not bite her tongue. She was “black in the face”.
In 1870 Jackson presented a lecture to the to the medical graduates of St. Andrews University in which he consolidated his experiences of unilateral seizures, and his interpretation of their implications for the understanding of brain function. A landmark paper in the filed of epileptology
Seizure Characterisation
Jackson studied seizures marked by deliberate, progressive spasm affecting one side of the body, with different parts involved sequentially. He classified these seizures based on the initial site—hand, face/tongue, then foot—mirroring the pattern described by Bravais.
Differences from Bravais
- Bravais described the clinical pattern but not the underlying mechanisms.
- Jackson emphasised the progressive spread of the convulsions and included bilateral involvement (e.g., trunk muscles, contralateral side) under the same seizure type.
- Jackson also recognised that loss of consciousness could occur before the spread to the second side.
Pathophysiological Insights
Unlike Bravais, Jackson linked seizures to cortical pathology, specifically:
- Instability of the grey matter in convolutions of the opposite hemisphere
- Focus on areas anatomically related to the corpus striatum (then thought to generate pyramidal tracts)
- Localisation of motor function in the cortex supplied by the middle cerebral artery
Experimental Confirmation
Jackson’s ideas were experimentally validated by Fritsch and Hitzig (1870), who demonstrated cortical localisation of motor function in dogs.
Impact on Epileptology
Jackson generalised his findings to all forms of epilepsy, thereby:
- Challenging earlier notions that seizures originated in the brainstem
- Establishing the foundations of modern epileptology
But as ever, if you go back far enough, there is usually an older description…
If at the time of his possession, while he is sitting down, his (left) eye moves to the side, a lip puckers, saliva flows from his mouth, and his hand, leg and trunk on the left side jerk (or, twitch) like a (newly)-slaughtered sheep, it is miqtu. If at the time of the possession his mind is consciously aware, (the demon) can be driven out; if at the time of the possession his mind is not so aware, (the demon) cannot be driven out.
Wilson JVK, Reynolds EH. (1990) [Babylonian Sakkiku 1050BC]
Jackson syndrome (1872)
A brainstem disorder consisting of homolateral ninth, tenth, and twelfth cranial nerve palsies (anaesthesia of the pharynx and larynx, paresis of the soft palate, and of the tongue), and contralateral hemiparesis. Most often associated with a medullary tegmental stroke or tumour.
In 1872 Hughlings Jackson reported the case of a 51 year old male he first examined in 1864 following a stroke in 1861. One of a series of cases “in which there is palsy, partial or complete, of one or more of the factors concerned in articulation, deglutition, and vocalisation“
Sir Stephen Mackenzie (1844–1909) reported two cases of unilateral bulbar paresis in 1886. The two syndromes are considered sufficiently alike to allow their eponymous fusion as Jackson-MacKenzie syndrome
Jackson cerebellar syndrome (‘fits’)
A syndrome of seizures caused by midline cerebellar tumour. The seizures are sometimes preceded by a loud cry. The head is drawn back and back curved, hands clenched, forearms flexed, legs extended, feet arched backward. A persistent hyperextended posture remains present between the attacks (cerebellar attitude)
Cerebellar seizures were first described by Johann Paul Wurffbain (1655-1711) in a 2 year old girl
…the neck was bent in the form of a bow and, being drawn backwards onto the back with great violence and resting on the shoulder blades, there stuck whilst the unhappy infant kept screaming…the symptoms being identical with that of the type of convulsion traditionally styled opisthotony
Wurffbain, 1691. Leopold Academy of Nuremberg
1871 – Jackson presented the case of a 5-year-old boy with a 4-month history of “tetanus-like seizures” secondary to a tubercular abscess of the middle lobe of the cerebellum in the BMJ Hospital Reports
….sometimes but not always the seizure was preceded by a loud cry… There was no marked twitching of the face, nor any special deviation of the eyeballs. His hands were clenched; his forearms were flexed on the upper arms, which were generally kept to the sides…The head was drawn back and the back was curved…The legs were always extended to the fullest possible degree, the feet being arched backwards …
Jackson 1871
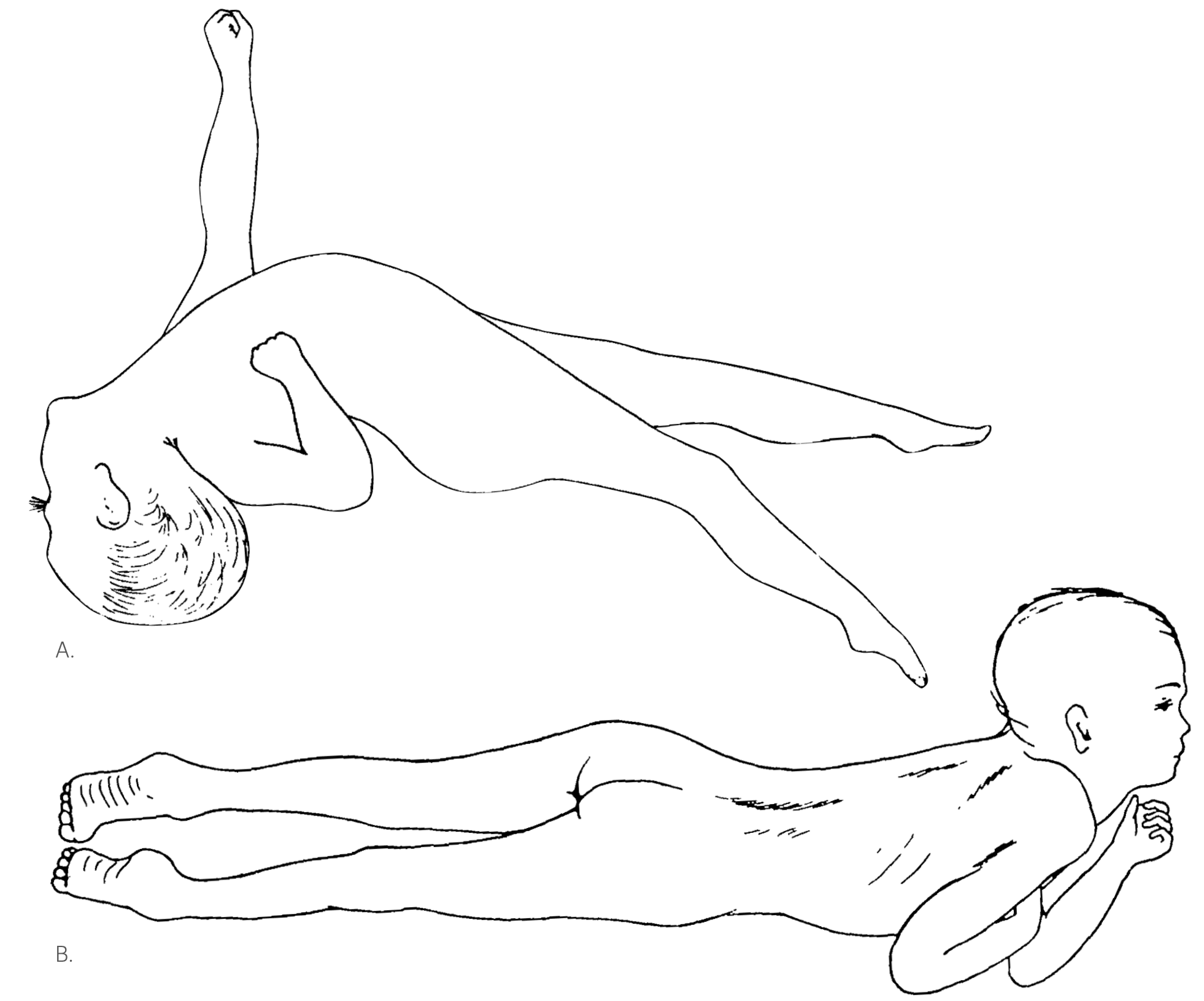
Unfortunately, a sketch of this patient’s attitude in the state of paralysis with rigidity and another sketch of him whilst he was having tetanus-like seizures, sketches exhibited when the paper was read, were not published with the report. They are appended in this report
Jackson 1907
Jackson’s Laws/Axioms
- “Those neural functions that are most lately developed are also the first to be lost.”
- For example after epileptic attacks, simple nervous processes are more quickly regained than are complex ones. (Jackson’s rule)
- “The study of the causes of things must be preceded by the study of things caused.“
- “The brain knows nothing of muscles, it only knows movements”
- Attributed to Charles Edward Beevor (1854-1908) as Beevor’s axiom (1898). However Beevor ascribed authority to Jackson in his future papers using this phrase
Here I may best remark on the differences between muscles and movements, a matter of vast importance. To speak figuratively, the central nervous system knows nothing of muscles, it only knows movements.
Jackson 1899
Major Publications
- Jackson JH. Unilateral epileptiform seizures, attended by temporary defect of sight. The Medical times and gazette 1863; 1: 588-589 [Jacksonian march]
- Jackson JH. Illustrations of diseases of the nervous system. Clinical lectures and reports by the medical and surgical staff of the London Hospital. 1864; 1: 337-388
- Jackson JH. Note on the comparison and contrast of regional palsy and spasm. Lancet 1867; 89(2271): 295-297
- Jackson JH. A study of convulsions. St. Andrews Medical Graduates’ Association. 1870
- Jackson JH. Case of tumour of the middle lobe of the cerebellum. Br Med J 1871; 2: 528-529
- Jackson JH. On a case of paralysis of the tongue from haemorrhage in the medulla oblongata.
Lancet 1872; 100(2570): 770-773 [Jackson syndrome] - Jackson JH. Contribution to the comparative study of convulsions. Brain 1886; 9: 1-23.
- Jackson JH. On a Particular Variety of Epilepsy (“Intellectual Aura”), One Case with Symptoms of Organic Brain Disease. Brain 1889; 11: 179–207.
- Jackson JH. Case of tumour of the middle lobe of the cerebellum — cerebellar paralysis with rigidity (cerebellar attitude) — occasional tetanus-like seizures (1871). Brain 1907; 29:425-440
References
Biography
- Head H. Hughlings Jackson on aphasia and kindred disorders of speech. Brain 1915; 38: 1–42.
- Taylor J. The ophthalmological observations of Hughlings Jackson and their bearing on nervous and other diseases. Brain 1915; 38: 391–417
- Walshe FMR. Contributions of John Hughlings Jackson to neurology: a brief introductions to his teachings. Arch Neurol 1961; 5: 119–31.
- York GK, Steinberg DA. An introduction to the life and work of John Hughlings Jackson with a catalogue raisonné of his writings. Med Hist Suppl. 2006;(26):3-157.
- Silvester A. Jean Martin Charcot (1825-93) and John Hughlings Jackson (1835-1911): neurology in France and England in the 19th century. J Med Biogr. 2009;17(4):210-3.
- Swash M. John Hughlings Jackson (1835-1911): An adornment to the London Hospital. J Med Biogr. 2015;23(1):2-8
Eponymous terms
- Wurffbain JP. OBSERVATIO CCXXVII: Hydrocephalo interno cum violentissima capitis tergum versus retractione convulsiva. Miscellanea curiosa, sive, Ephemeridum medico-physicarum Germanicarum 1689; 427-429
- Bravais LF. Recherches sur les symptômes et le traitement de l’épilepsie hémiplégique, Thèse, Paris, 1827.
- Todd RB. On the pathology and treatment of convulsive diseases. 1849
- Fritsch G, Hitzig E. (1870) Ueber die elektrische Erregbarkeit des Grosshirns. Archiv fur Anatomie und Physiologie 37:300–332.
- Charcot JM, Pitres A. Contribution à l’étude des localisations dans l’écorce des hémisphères du cerveau. Revue mensuelle de medicine et de chirugie 1877; 1: 1–18, 113–123, 180–195, 357–376, 437–457. [Épilepsie Bravais-Jacksonienne]
- Mackenzie S. Two cases of associated paralysis of the tongue, soft palate and vocal chord on the same side. Transactions of the Clinical Society of London 1886; 19: 317–9. [Jackson-Mackenzie Syndrome]
- Fulton JF. A case of cerebellar tumor with seizures of head retraction described by Wurffbain in 1691. The Journal of Nervous and Mental Disease, Baltimore, 1929; 70(6): 577-583
- Taylor DC, Marsh SM. Hughlings Jackson’s Dr Z: the paradigm of temporal lobe epilepsy revealed. J Neurol Neurosurg Psychiatry. 1980 Sep;43(9):758-67.
- Eadie MJ. The evolution of J. Hughlings Jackson’s thought on epilepsy. Clin Exp Neurol. 1990;27:29-41.
- Wilson JVK, Reynolds EH. Translation and analysis of a cuneiform text forming part of a Babylonian treatise on epilepsy. Med Hist 1990; 34: 185–198. [Jacksonian March]
- Kennedy PG. Philosophical aspects of John Hughlings Jackson’s ideas on speech disorders and the nervous system. J Med Biogr. 1997 Feb;5(1):17-21.
- Meares R. The contribution of Hughlings Jackson to an understanding of dissociation. Am J Psychiatry. 1999 Dec;156(12):1850-5.
- York GK 3rd, Steinberg DA. Hughlings Jackson’s suggestion for the treatment of epilepsy. Neurology. 2009 Oct 6;73(14):1155-8
- Eadie M. Louis François Bravais and Jacksonian epilepsy. Epilepsia. 2010 Jan;51(1):1-6. [Jacksonian epilepsy]
- York GK 3rd, Steinberg DA. Hughlings Jackson’s neurological ideas. Brain. 2011 Oct;134(Pt 10):3106-13.
- Iniesta I. John Hughlings Jackson and our understanding of the epilepsies 100 years on. Pract Neurol. 2011;11(1):37-41
- York GK 3rd. Hughlings Jackson on joking. Brain. 2015 May;138(Pt 5):1435-9
Eponym
the person behind the name
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |