
![]()
John T. Bowen

John Templeton Bowen (1857-1940) was an American dermatologist.
Pioneer of dermatopathology and first professor of dermatology at Harvard Medical School.
Most famous for his description of ‘precancerous dermatoses’ published in the Journal of Cutaneous Diseases in 1912. Eponymously associated with carcinoma in situ or intraepithelial neoplasia of sun exposed skin (Bowen’s disease); vulva (Bowen’s disease of the vulva); and penis (Bowenoid papulosis and Bowen’s disease of the penis)
Biography
- Born on July 8, 1857 in Boston
- 1869–1875 Studied at America’s oldest school, the Boston Latin School
- 1879 – BA, Harvard College
- 1884 – MD, Harvard Medical School
- 1884-1887 Post-graduate dermatology training in Berlin, Munich and Vienna
- 1889 – Assistant physician for Diseases of the Skin to the Massachusetts General Hospital serving the Harvard Medical School. Full physician in 1895
- 1896 – Instructor in dermatology, Harvard Medical School
- 1907 – First Edward Wigglesworth Professor of Dermatology of the Harvard University
- 1912 – Emeritus Professor of Dermatology
- Died on December 3, 1940
Medical Eponyms
Bowen’s disease (1912)
Bowen’s disease is an intra-epidermal squamous cell carcinoma or squamous cell carcinoma in situ. It occurs when a collection of squamous cells in the outer skin layer (epidermis) become cancerous. They appear as red scaly patches on the skin surface. They are typically slow-growing but if left untreated may progress to invasive squamous cell carcinoma. It most commonly affects sun exposed areas of skin.
1912 Bowen first described the disease, that later became named after him. He reported two cases, both males in their 50’s with skin eruptions described as ‘chronic atypical epithelial proliferation’.
The lesions were circumscribed; in the one case limited to the left gluteal region, in the other to the calf of the right leg. They appeared as papular and tubercular lesions, only slightly elevated above the normal skin, of a moderately firm consistency, and dull red in color. The surface was in some places slightly crusted; in other places it had a papillomatous character. The lesions were in places confluent, forming areas of tumor-like masses; in other places, especially at the edge of the affected areas, they were discrete, or assumed annular or serpiginous figures.
As yet no signs of malignancy have appeared in these cases. It can hardly be doubted that such a sequel is imminent.
Bowen, 1912
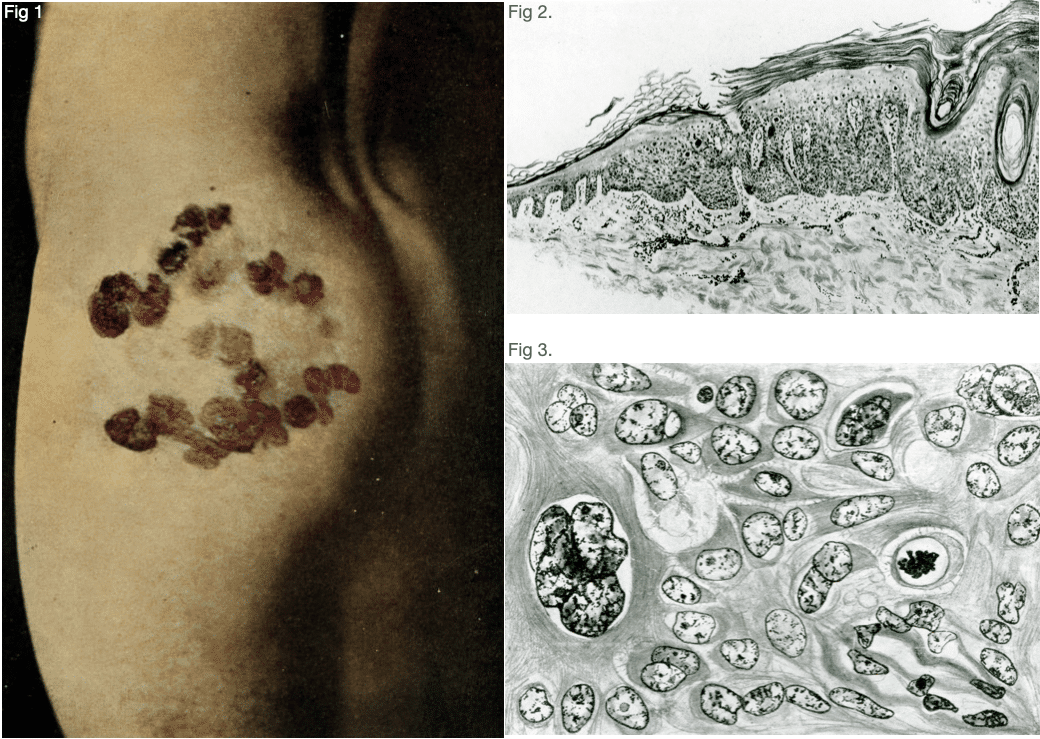
Bowen. Case 1 (Fig 103) In: Precancerous Dermatoses. 1912
Fig. 1. As it appeared in October, 1911. The cicatricial portions mark the site of lesions previously removed.
Fig. 2. Low power shows hyperkeratosis, proliferation and thickening of rete, vacuolization and abnormal cornification of cells; dilatation of vessels of corium, with cell masses surrounding them.
Fig. 3. High power. Shows peculiar “clumping” of nuclei and karyokinesis
1914 The subject was greatly elaborated and clarified by Ferdinand-Jean Darier (1856-1938) in an article in the Annales de dermatologie et de syphiligraphie titled la dermatose précancéreuse de Bowen, dyskératose lenticulaire et en disques in which is embodied the description of a further three typical examples of the same affection.
1915 Bowen followed up his original contribution reviewing his first two cases; then the three cases of Darier and Danel; and finally adding a third case of his – the sixth case to be reviewed. Bowen’s final review was published in Archives of Dermatology in 1920
1918 Darier included the disease in his Textbook of Dermatology as ‘Dyskeratosis of Bowen’. He included a photograph of the skin lesion he had seen on the ankle of a 39-year-old female.
Original
English
Dermatose précancéreuse de Bowen ou dyskératose lenticulaire et en disques. – J’ai proposé d’attacher le nom de J.T. Bowen à une dermatose essentiellement chronique et progressive, qu’il a le premier décrite en 1912. Elle se présente sous forme de disques lenticulaires ou nummulaires (Fig 77), puis de placards de forme irrégulére, surmontés d’épaisses squames-croûtes; les éléments généralement multiples, non symétriques, peuvent siéger n’importe où. On peut rencontrer aussi des taches atrophiques, d’apparence pagetoide.
Darier 1918 (French 2e)
Precancerous Dermatosis of Bowen or Dyskeratosis Lenticularis et Discoides. – I have recommended that the name of J. T. Bowen be attached to an essentially chronic and progressive dermatosis first described by him in 1912. It appears in the form of lenticular or nummular disks (Fig. 80), later patches of irregular shape, covered with thick scaly crusts; the lesions are generally multiple, non-symmetrical, and may be situated anywhere. Atrophic spots, resembling Paget’s disease, may also be seen.
Darier 1920 (English translation of French 2e)

Bowen’s disease of the vulva [aka vulvar intraepithelial neoplasia ]
Bowen’s disease is regarded as a squamous-cell carcinoma in situ, and can develop on any part of the skin surfaces or mucous membranes. The majority are cases occur on sun-exposed surfaces such as the head, neck, and hands. Lesions on the vulva are less common.
In 1943, Richard van Dyck Knight reviewed the literature on Bowen’s disease of the vulva, traced reports of 26 cases, and added 6 new ones. He concluded that Bowen’s disease was
…a specific entity, namely, a superficial, noninvasive intraepithelial epithelioma characterized by (a) Chronicity, pruritus and a characteristic gross and microscopic appearance and (b) Malignant tendencies when involving mucosal surfaces.
Knight, 1943
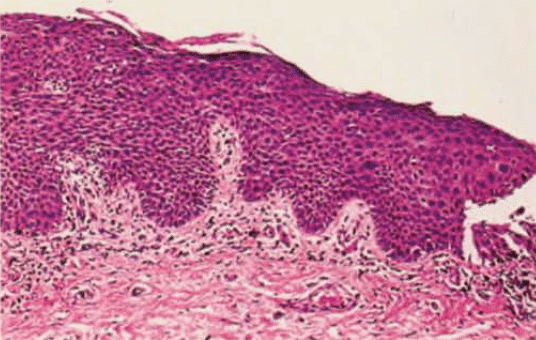
Subsequent evaluation confirmed the characteristics of Bowen’s disease as epidermal hyperplasia; parakeratosis; mitotic figures (especially in the upper 1/2 to 1/3 of the epidermis); and atypical keratinocytes with large hyperchromatic, pleomorphic nuclei and multinucleated keratinocytes.
Human papillomavirus (HPV) type 16 and related types are frequently found in genital located Bowen’s disease and only rarely identified in non-genital cutaneous Bowen’s disease and squamous cell cancer (SCC). In 1983, Ikenberg et al found that HPV 16 DNA or related sequences were identified in 60% of cases of Bowen’s disease (80% in cases of genital localization); and in 80% biopsies from Bowenoid papulosis.
…these data reveal a striking association of HPV 16 infections with both types of lesion which are generally regarded as precancerous conditions…the very specific presence of HPV 16 DNA in Bowen’s disease and Bowenoid papulosis and in human genital cancer of three different sites (cervical, vulva and penile) points to some role of these infections in the induction of these proliferative changes.
Ikenberg et al, 1983
In 1987 the term was “deleted from the vocabulary of vulvar diseases” by gynecopathologists and was substituted by the non-specific designation “vulvar intraepithelial neoplasia”
Bowenoid papulosis
Bowenoid papulosis is a sexually transmitted condition occuring in both males and females that presents as pigmented genital papules due to human papillomavirus (HPV) infection, particularly HPV 16. Now more commonly termed vulvar or penile squamous intraepithelial lesion or High grade squamous intraepithelial lesion (HSIL).
HSIL is a squamous cell abnormality associated with human papillomavirus (HPV) and encompasses the entities previously termed cervical intraepithelial neoplasia (CIN), and carcinoma in situ. HSIL has the potential to become invasive squamous cell carcinoma.
In 1977, Kopf and Bart described Bowenoid papules of the penis as a potential new clinical entity. They presented a case of a young man with multiple papules on the shaft and glans of his penis. Histology showed many discrete lesions of squamous cell carcinoma in situ (Bowen’s disease) concentrated in a small area.
1978, Wade et al studied 36 biopsy specimens from 11 men aged 21-36 years presenting with multiple red-violaceous papules, some distinctly verrucoid or velvety on either or both the shaft and glans of the penis. The clinical diagnoses accompanying the biopsy specimens included lichen planus, psoriasis and condyloma acuminatum. In no instance was carcinomia in situ suggested in the differential diagnosis. Histologically, however, all specimens submitted showed indubitable changes of squamous cell carcinoma in situ. Bowenoid papulosis (BP)shares the histological features of Bowen’s disease of the penis (BPD) but is distinguished from the latter by clinical differences
1) onset at a much earlier age (average age of 28), 2) multiple simultaneous lesions in all patients, 3) localization primarily on the shaft rather than the glans of the penis, 4) lack of symptoms, 5) smaller size (2 mm to 10 mm), 6) papules rather than plaques, and 7) verrucoid nature of some lesions
Wade, 1978
Note: There is confusion in nomenclature of three clinical variants of carcinoma in situ of the penis. Histopathologically, these conditions share similar histologic features of squamous cell carcinoma in situ, but the clinical features and presentations differ.
- Bowenoid papulosis (BP): Multiple wart-like lesions, often pigmented in keratinized sites, and more numerous and more inflamed at ‘mucosal’ sites. The lesions are smoother (less papillomatous), polymorphic and more coalescent than common genital viral warts (condylomata acuminata). They occur in young, sexually active men
- Bowen’s disease of the penis (BDP): Red or hyperpigmented scaly patches and plaques of the keratinised penis often with a warty or crusty appearance. More common in older males.
- Erythroplasia of Queyrat (EQ): Single or multiple, non-tender, shiny red patches or plaques of the ‘mucosal’ penis. More common in older males. Originally described and drawn by Auguste Queyrat in 1911
Major Publications
- Bowen JT. On the occurrence of small-pox lesions in the internal organs. Reprint from Vierteljahresschrift für Dermatologie und Syphilis. 1887. 4
- Bowen JT. On the occurrence of small-pox lesions in the internal organs: with some studies of the skin eruption. 1888
- Bowen JT. The Epitrichial Layer of the Human Epidermis. Anatomischer Anzeiger 1889; 13,14: 412-416; and 441-450
- Bowen JT. Cases of cutaneous tuberculosis, with histological studies. Journal of cutaneous and genito-urinary diseases. 1890
- Bowen JT. The association of purpura and acute circumscribed oedema. Journal of cutaneous and genito-urinary diseases. 1892
- Bowen JT. Hydroa vacciniforme, bazin, Hutchinson’s summer eruption. Journal of cutaneous and genito-urinary diseases 1894.
- Bowen JT. The epitrichial layer of the epidermis and its relationship to ichthyosis congenita. New York 1895.
- Bowen JT. Keratosis follicularis (psorospermose folliculaire végétante, Darier), apropos of a new case. Journal of cutaneous and genito-urinary diseases 1896.
- Bowen JT. Congenital bullous dermatitis with epidermic cysts. 1898
- Bowen JT. Precancerous dermatoses: A study of two cases of chronic atypical proliferation. The Journal of Cutaneous Diseases Including Syphilis, New York 1912; 30: 241-255
- Bowen JT. Precancerous dermatoses: a sixth case of a type recently described. The Journal of Cutaneous Diseases Including Syphilis, New York, 1915; 33(12): 787-801
- Bowen JT. Precancerous dermatoses: the further course of two cases previously reported. Arch Derm Syphilol 1920; 1: 23–4.
- Bowen JT. Centennial paper: Precancerous dermatoses: A study of two cases of chronic atypical proliferation. Arch Dermatol. 1983;119(3):243-260
References
Biography
- White CJ. John Templeton Bowen, MD 1857-1940. Arch Derm Syphilol. 1941; 43(2): 386-388
- Graham-Little E. Obituary: John Templeton Bowen. Br J Dermatol 1941; 53(6): 190–1.
- Weyers W. The centennial of Bowen’s disease-a critical review on the occasion of the 100th anniversary of its original description. Dermatol Pract Concept. 2012 Oct 31;2(4):204a02.
- Ali H, Shipman AR, Orpin SD. John Templeton Bowen, MD, 1857-1940: the centenary of his most famous publication. Clin Exp Dermatol. 2012 Oct;37(7):825-8.
- Arora H, Arora S, Shah V, Nouri K. John Templeton Bowen. JAMA Dermatol. 2015 Dec 1;151(12):1329
- Baskett TF. Bowen, John Templeton (1857–1940) In: Eponyms and Names in Obstetrics and Gynaecology. 3e. 2019
- Bibliography. Bowen, John T. (John Templeton). WorldCat Identities
Eponymous terms
Bowen’s disease
- Darier J. La dermatose précancéreuse de Bowen, dyskératose lenticulaire et en disques. Annales de dermatologie et de syphiligraphie 1914; 5(8): 449-471
- Darier J. A text-book of dermatology. 1920 [English translation of French 2e, 1918] [Bowen disease pp236]
- Bernhard JD, Elliot AD. A Letter From Darier to Bowen on the Naming of Bowen’s Disease. Arch Dermatol. 1983;119(3):261-262
Bowen’s disease of vulva
- Knight R. van D. Bowen’s disease of the vulva. American Journal of Obstetrics and Gynecology. 1943; 46(4): 514-524
- Leckie FH. Bowen’s disease of the vulva; report of 2 cases. J Obstet Gynaecol Br Emp. 1955 Apr;62(2):288-90.
- Ikenberg H, Gissmann L, Gross G, Grussendorf-Conen EI, zur Hausen H. Human papillomavirus type-16-related DNA in genital Bowen’s disease and in Bowenoid papulosis. Int J Cancer. 1983 Nov 15;32(5):563-5.
- Kaufman RH, Friedrich EG, Jr., Woodruff JD. New nomenclature for vulvar disease. Obstet Gynecol. 1976 Jan;47(1):122-4.
- Ridley CM, Frankman O, Jones IS, Pincus SH, Wilkinson EJ, Fox H, Friedrich EG Jr, Kaufman RH, Lynch PJ. New nomenclature for vulvar disease: International Society for the Study of Vulvar Disease. Hum Pathol. 1989 May;20(5):495-6
Bowenoid papulosis
- Queyrat L. Erythroplasie du gland. Bulletin de la Société française de dermatologie et de syphiligraphie. 1911; 22: 378-382
- Kopf AW, Bart RS. Tumor conference No. 11: multiple bowenoid papules of the penis: a new entity? J Dermatol Surg Oncol. 1977 May-Jun;3(3):265-9
- Wade TR, Kopf AW, Ackerman AB. Bowenoid papulosis of the penis. Cancer. 1978 Oct;42(4):1890-903
- Singhal RR, Patel TM, Pariath KA, Vora RV. Premalignant male genital dermatoses. Indian J Sex Transm Dis AIDS. 2019 Jul-Dec;40(2):97-104
Eponym
the person behind the name

Welsh junior doctor graduated from Cardiff Medical School with MBBCh and BSc in Medical Education. Currently working in emergency medicine in Perth, Australia. Aim to commence GP training in the UK in 2022.