
![]()
Karel Maydl
Karel Maydl (1853-1903) was a Czech surgeon
Karel (Carl) was a surgeon whose innovations influenced abdominal, urological, and orthopedic surgery. Educated at Charles University in Prague, he trained under Eduard Albert and later succeeded him as professor of surgery at Innsbruck and Prague. Renowned as a brilliant teacher and operator, Maydl combined meticulous anatomical knowledge with a constant drive to improve surgical safety and technique.
He contributed original operations and descriptions that have become enduring eponyms. In 1895, he provided the first pathological account of femoral head necrosis in adolescents, a condition later rediscovered and named Legg–Calvé–Perthes disease. In 1888, he revolutionised colostomy by introducing complete bowel division and spur formation, eliminating the stagnant blind loop. In 1894, his method for bladder exstrophy proposed ureteral implantation into the sigmoid colon — a bold precursor of modern urinary diversion. And in 1898, he described the W-shaped loop strangulation that bears his name as Maydl’s hernia.
Despite his early death at just 50 years of age, Maydl left a profound mark on European surgery. His techniques advanced the management of complex abdominal, colorectal, and urological conditions, while his careful clinical observations shaped understanding of hip pathology in children. Buried at Olšany Cemetery in Prague, his legacy endures not only through the eponyms that bear his name but also through the surgical principles of safety, precision, and innovation that continue to guide practice today
Biographical Timeline
- Born March 10, 1853 in Rokytnice nad Jizerou, Bohemia (then Austrian Empire; now Czech Republic).
- 1871–1877 – Studied medicine at Charles University, Prague.
- 1878 – Received medical doctorate. Assistant at the surgical clinic under Eduard Albert (1841–1900).
- 1882 – Habilitation in surgery. Appointed associate professor at Prague.
- 1887 – Appointed Professor of Surgery, University of Innsbruck.
- 1891 – Returned to Prague as Professor of Surgery and Director of the Surgical Clinic, Charles University.
- 1892 – Described the W-shaped intestinal strangulation hernia (later called Maydl’s hernia).
- 1893 – First to perform subtotal colectomy for diffuse colonic disease; pioneer in urinary diversion and ureteral implantation.
- 1897–1902 – Published influential surgical works on abdominal and urological surgery, including intestinal resections and bladder reconstruction.
- Died August 8, 1903 in Dobřichovicích, aged 50. Buried at Olšany Cemetery, Prague, in a family tomb designed by Jan Kotěra with sculpture by Bohumil Kafka
Medical Eponyms
Maydl’s hernia (1898)
A rare form of strangulated internal hernia in which two adjacent bowel loops lie within the hernia sac, while the central intra-abdominal loop becomes strangulated, also known as the “W-shaped hernia”. Estimated to occur in 2–10% of strangulated hernias found more frequently in inguinal hernias, but also in femoral and incisional sites. Mortality in older case series was high (up to 40–50%), but outcomes improved with earlier recognition and resection.
High risk of missed diagnosis as the external hernia sac may appear viable while the intra-abdominal loop is necrotic. Recognising the “W-configuration” intraoperatively is crucial and resection of the central loop is required, not just reduction of the visible hernia.
1895–1898, Maydl described the condition and presented his cases in Prager medizinische Wochenschrift. He highlighted the clinical paradox that the strangulated, ischaemic loop lies within the abdominal cavity, while the hernia sac itself may appear only partially compromised. Failure to recognise this concealed intra-abdominal strangulation leads to delayed diagnosis and high mortality.
Original
English
Ich habe unter meinen Bruchoperationen zwei Fälle beobachtet, in denen eine W-förmige Lage der Darmschlingen vorlag. Die beiden äußeren Schlingen lagen im Bruchsacke, die mittlere war im Abdomen zurückgeblieben, und gerade diese innere Schlinge verfiel zuerst der Gangrän – Maydl 1898
In my hernia operations I have observed two cases in which there was a W-shaped arrangement of the intestinal loops. The two outer loops lay in the hernia sac, the middle remained within the abdomen, and it was precisely this inner loop that first fell into gangrene – Maydl 1898
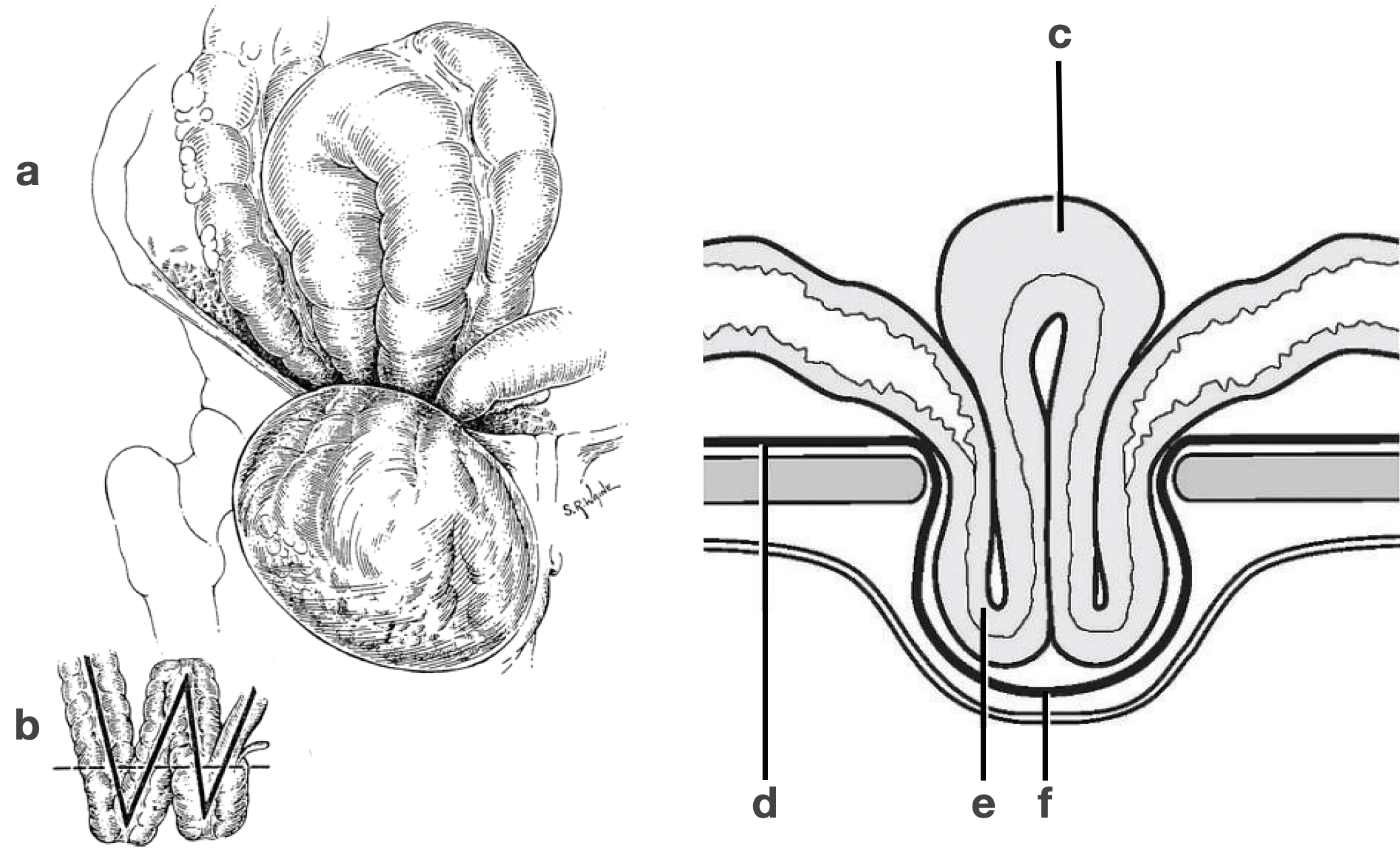
Obstructed loop of intestine within peritoneal cavity d) Peritoneum e) Hernia contents f) Hernia sac
Maydl’s Operation (1883 Colostomy)
Colostomy (anus praeternaturalis) had been attempted since the first hypothetical proposal in 1710 by Alexis Littré (1654-1726) and first recorded attempt was made by Pillore of Rouen in 1776. In the 19th century, surgeons debated the safest and most functional technique e.g. peritoneal vs. lumbar, or one-stage vs. two-stage.
While assistant to Eduard Albert (1841–1900) in Vienna, Maydl became dissatisfied with the “wall-fixed” colostomy, in which only part of the bowel circumference was sutured. He observed frequent stasis, enteritis, and ulceration in the blind loop, requiring repeated artificial evacuation.
1883 – Maydl proposed and began performing a new method in which the bowel was completely divided, with the proximal and distal ends both brought out and fixed to the abdominal wall. A spur was created by passing a gauze strip through the mesocolon, separating the afferent and efferent limbs. This ensured complete diversion of stool and eliminated the problem of stagnation in the distal segment.
Original
English
Anstatt nur einen Theil des Darmumfanges zu fixiren, soll man den Darm vollständig durchtrennen und die ganze Peripherie sowohl des oberen als auch des unteren Endes an die Haut nähen. … Auf diese Weise wird die Operation zwar etwas complicirter, aber sicherer, und ihr Nutzen ein dauernder – Maydl 1888
Instead of fixing only a portion of the bowel circumference, one should divide the intestine completely, and suture the entire periphery of both upper and lower ends to the skin… In this way the operation is somewhat more complicated, but certainly safer, and its benefit permanent. – Maydl 1888
By 1886 he had performed the operation more than a dozen times, including cases of rectal carcinoma, cicatricial stenosis, and congenital atresia. The technique was adopted in Albert’s surgical textbook and disseminated internationally.
Maydl’s Method
Surgical technique for exstrophy of the bladder (ektopia vesicae urinariae).
1894 – Maydl described the first attempt at a radical surgical treatment of bladder exstrophy. This involved total extirpation of the bladder with the implantation of both ureters into the sigmoid colon (flexura sigmoidea), allowing urine to drain into the large intestine.
This procedure was pioneering in concept but associated with a high morbidity. It represented the earliest systematic attempt to restore continence in exstrophy, moving beyond mere cutaneous coverings or diversions.
Maydl’s method laid the foundation for modern urinary diversion and ureterosigmoidostomy with his work influencing later innovators including Simon, Coffey, and Leadbetter.
Key Medical Contributions
Legg-Calvé-Perthes disease (LCPD)
Pediatric hip disorder caused by avascular necrosis of the femoral head, typically in children aged 5–10. It progresses from ischemia and collapse of the epiphysis through revascularisation and remodelling, leading to deformity, stiffness, limp, and risk of early osteoarthritis.
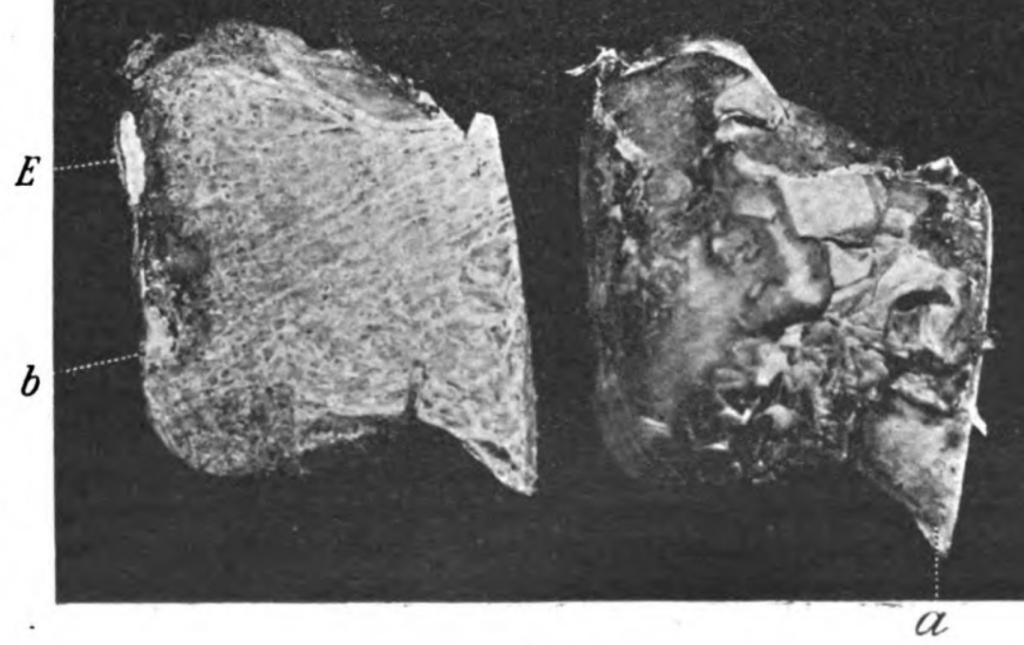
1897 – Maydl first publishes on two cases of arthritis deformans coxae in adolescent patients. He illustrated resected femoral heads from two adolescents (Fig. 1 and 2). Both show the characteristic flattening, osteophytes, and resorption changes now recognised as Legg–Calvé–Perthes disease.
Original
English
..im Jahre 1895 Erkrankungsfälle der Hüftgelenksgegend zu untersuchen Gelegenheit hatte, die einer coxa vara in vielfacher Beziehung ungemein ähnlich, doch nicht als solche aufgefasst werden konnten, sich auch nach einem therapeutischen operativen Eingriffe nicht als solche erwiesen… Wenn auch die traumatische Arthritis deformans eine allgemein bekannt Erkrankung ist, so ist dieselbe bei adolescenten Leuten eine recht seltene Erscheinung und in ihrem klinischen und anatomischen Aussehen recht wenig bekannt.
F.B., 15jährige Schneiderstochter aus Zeltschan, aufgenommen am 16. Mai 1895, gibt folgendes als Anamnese an:…Vor einem Jahre rutschte der Kranken beim Stiegenabwärtsgehen das rechte Bein aus, die Kranke glitt auf der rechten Seite liegend etwa 6 Stufen abwärts…- Maydl K. 1897
…in 1895, had the opportunity to examine cases of hip joint disease that were remarkably similar to coxa vara in many respects, yet could not be considered as such… Although traumatic arthritis deformans is a generally recognized disease, it is a rare occurrence in adolescents and relatively little known in its clinical and anatomical appearance.
Case 1: F.B., a 15-year-old tailor’s daughter presents a year after an injury. Her right leg slipped while descending stairs and, lying on her right side, she slid down six steps…- Maydl K. 1897
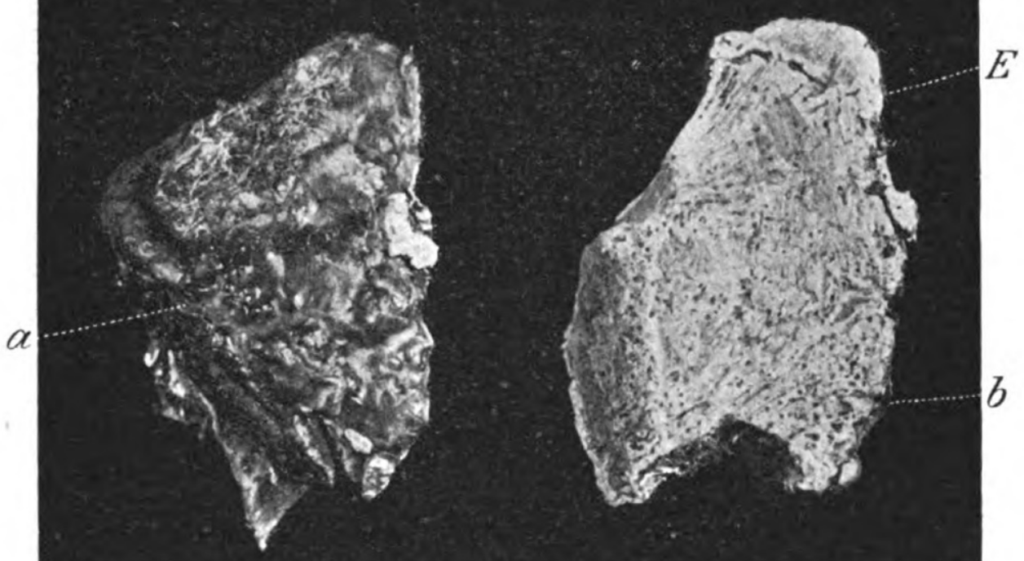
LEFT: Figure 1 (a, b). Resected femoral head from a 15-year-old girl with arthritis deformans coxae. Head markedly flattened, broadened, and vertically elongated. Pear-shaped contour with narrowing superiorly. Surface and rim covered with wart-like, comb-shaped osteophytes. Cartilage covering very thin.
RIGHT: Figure 2 (a, b). Resected femoral head from an 18-year-old miner. Head nearly flat rather than hemispherical. Articular surface extended posteriorly. Osteophytes present at the rim.
The letter “E” marks the deep resorption groove or notch that Maydl described: “…eine tiefe, halbkreisförmige Resorptionsrinne, concentrisch mit dem Mittelpunkte des Kopfes…” → “…a deep, semicircular resorption groove, concentric with the centre of the head…”.
Maydl and Unusual Hernia Contents (1895)
In 1895, Karel Maydl published “Ueber retrograde Incarceration der Tuba und des Processus vermiformis in Leisten- und Schenkelhernien” (Wiener klinische Rundschau 9: 17–19). In this short but significant paper, he described retrograde incarceration of the fallopian tube and the vermiform appendix within inguinal and femoral hernias. His careful pathological descriptions demonstrated that structures beyond the small bowel or omentum could be found within the sac — a finding that anticipated later recognition of “uncommon hernia contents.”
- Fallopian tube herniation: Maydl noted cases where adnexal structures (tube ± ovary) were found incarcerated within inguinal hernia sacs. Although pediatric surgeons later associated adnexal herniation with congenital anomalies, Maydl’s account provided one of the earliest adult descriptions.
- Appendix herniation: He also documented the appendix within hernia sacs — a precursor to what would later be eponymously tied to Amyand (inguinal) and De Garengeot (femoral) hernias.
Modern series confirm the rarity of these entities: a large review of 1,950 groin hernia repairs found fallopian tubes/ovaries in ~2.9%, and the appendix in ~0.5%. A recent 2024 case report again emphasized the importance of considering tubo-ovarian herniation, especially in adult women.
Though the term “Maydl’s hernia” is reserved for the W-shaped retrograde loop described later (1898), his 1895 contribution helped establish the broader category of “uncommon hernia contents”. Interestingly, while Amyand and De Garengeot secured eponymous recognition, fallopian tube herniation into the inguinal canal has never acquired an eponym — despite Maydl’s early report.
Major Publications
- Maydl C. Ueber Gastrostomie. 1882
- Maydl C. Über den Darmkrebs. 1883
- Maydl K. Zur Technik der Kolotomie. Centralblatt für Chirurgie, Leipzig, 1888, 15: 433-439. [Maydl’s operation]
- Maydl C. Über Echinokokkus der Pleura und die ihn vortäuschenden Localisationen der Echinokokkenkrankheit. 1891
- Maydl K. Ueber die Radikaltherapie der Ektopia vesicae urinariae. Wiener medizinische Wochenschrift, 1894; 44: 1113-1115, 1169-1172, 1209-1210, 1256-1258, 1297-1301. [Maydl’s method]
- Maydl K. Über subphrenische Abscesse. 1894
- Maydl K. Ueber Bruchschnitte, Prager Medicinische Wochenschrift, 1898; 23(3): 25–28
- Maydl C. Ueber retrograde Incarceration der Tuba und des Processus vermiformis in Leisten- und Schenkelhernien. Wiener klinische Rundschau 1895; 9(2): 17-19
- Maydl K. Coxa vara und Arthritis deformans coxae. Wiener klinische Rundschau 1897; 11: 153-154. [Legg-Calvé-Perthes disease]
- Maydl K. Die Lehre von den Unterleibsbrüchen (Hernien). Wien, Stefan, 1898. [Maydl’s hernia]
Controversies
Karel vs Carl
Maydl’s works appear under two forenames, Carl (German form) in his early career, and Karel (Czech form) in later years.
In the Austrian-German academic world of the 1870s–80s, he published as Carl Maydl e.g. Ueber Gastrostomie. From the 1890s onwards, he increasingly used the Czech form Karel Maydl, reflecting the Czech national movement and his own preference. Obituaries and Czech memorials (1903, 1953) consistently use Karel.
Both forms are correct in their historical context. Bibliographies should include Carl Maydl for earlier works and Karel Maydl for later publications. These are noted in the above publications as either Maydl C, or Maydl K.
References
Biography
- Redakce. MUDr. Karel Maydl. Časopis lékařů českých, 1903; 42(33): 861–863
- Jirasek A. Karel Maydl; k stému výrocí jeho narození [Karel Myadl; 100th anniversary of high birth]. Časopis lékařů českých. 1953; 92(11): 283-92.
- Karl Maydl 1853–1903. Dis Colon Rectum 2001; 44: 280–283
- Kokešová H. Chirurg Karel Maydl (1853–1903). Práce z dějin Akademie věd 2023; 2: 33-40
Eponymous terms
- Paul M. Maydl’s hernia. British Journal of Surgery, 1944; 32(125): 100–101
- Roberts PA. W-strangulation of bowel; the so-called Maydl’s hernia, or retrograde strangulation of intestine due to double loop incarceration. Guys Hosp Rep. 1954;103(3):265-8.
- Bayley AC. The clinical and operative diagnosis of Maydl’s hernia. A report of 5 cases. Br J Surg. 1970 Sep;57(9):687-90.
- Moss CM, Levine R, Messenger N, Dardik I. Sliding colonic Maydl’s hernia: report of a case. Dis Colon Rectum. 1976 Oct;19(7):636-8.
- Ganesaratnam M. Maydl’s hernia: report of a series of seven cases and review of the literature. Br J Surg. 1985 Sep;72(9):737-8.
- Narang R, Pathania OP, Punjabi P, Tomar S. Unusual Maydl’s hernia (a case report). J Postgrad Med. 1987 Jul;33(3):137-9.
- Weledji EP, Mokake M, Ngowe MN. A Rare Presentation of Maydl’s Hernia. Case Rep Surg. 2014;2014:184873.
- Hasnaoui A, Trigui R. A unique presentation of a strangulated epigastric Littre-Maydl hernia. ANZ J Surg. 2024 Mar;94(3):483-484
Eponym
the person behind the name
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |
Hola!
Muy emocionada leo varias veces la historia de mi bisabuelo Karl Maydl Perzina.
Investigo cada movimiento, cada palabra, para saber más de mi querido bisabuelo Karel.