
![]()
Kerley lines
Description
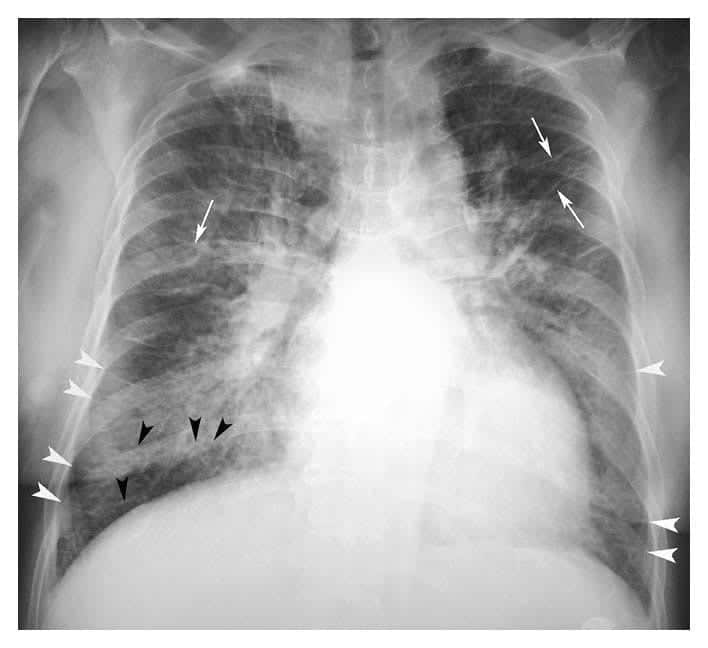
Kerley lines are described as types A, B or C.
- Kerley A lines are linear opacities extending from the periphery to the hila caused by distention of anastomotic channels between peripheral and central lymphatics
- Kerley B lines are small, horizontal, peripheral straight lines demonstrated at the lung bases that represent thickened interlobular septa on CXR. They represent edema of the interlobular septa and though not specific, they frequently imply left ventricular failure
- Kerley C lines are reticular opacities at the lung base, representing Kerley’s B lines end on (‘en face’).
History of Kerley lines
1933 – Peter James Kerley first described horizontal lines that he postulated to be peri-vascular lymphatics in patients with mitral stenosis and left ventricular failure.
Passive hyperaemia of the of the lungs caused by mitral stenosis or heart failure gives remarkable and very varied x-ray appearances. A severe attack of hyperaemia always leaves permanent radiologic evidence behind it…the shadows of perivascular lymphatics persist as fine, sharp lines, most marked at the bases and near the hila.
[BMJ 1933;2:594–597]
1951 – Kerley later differentiated these as ‘lines A, B, and C‘
‘These abnormal lines … are about .5–1 [millimeters] wide. They are of three types. (A) Lines several inches long, rather ragged and radiating from the hilum. They do not bifurcate and they do not follow the normal branching pattern of bronchi and vessels. (B) Short, sharp lines seen only at the bases, usually less than an inch long and running transversely out to touch the pleural margin. (C) Fine interlacing lines giving the network appearance. It is the fine interlacing lines which have given rise to the term reticulation.‘
1954 – FG Fleischner further investigated and determined ‘lines B’ represented thickened interlobular septa
1967 – ER Heitzman concluded that ‘lines A and C’ also represented thickened interlobular septa
‘…the concept is advanced that [lines A, B, and C] all represent manifestations of thickened interlobular septa. Each presents a different [radiologic] pattern due to different arrangement of the connective tissue septa in various parts of the lung.’
1954 – First eponymous use of ‘lines B of Kerley‘ made by JH Carmichael. – reported a high correlation between Kerley B lines and elevated pulmonary artery pressures in patients with mitral valve stenosis
1963 – DH Trapnell encouraged the use of the eponym, and it has remained.
Associated Persons
- Sir Peter James Kerley (1900-1979)
- Felix George Fleischner (1893-1969)
Alternative names
- Fleischner’s lines
- Linear X-ray shadows
- Septal lines, interlobular lines and basal horizontal lines
References
Original articles
- Kerley P. Radiology in heart disease. BMJ 1933; 2: 594–597
- Shanks EW, Kerley P. A Text-Book Of X-Ray Diagnosis: Vol II. W. B. Saunders. 1951: 403–415
- Fleischner FG, Reiner L. Linear x-ray shadows in acquired pulmonary hemosiderosis and congestion. N Engl J Med. 1954 May 27;250(21):900-5.
- Carmichael JH, Julian D, Jones G. Radiological signs in pulmonary hypertension; the significance of lines B of Kerley. Br J Radiol. 1954 Jul;27(319):393-7
- Trapnell DH. The peripheral lymphatics of the lung. Br J Radiol. 1963 Sep;36:660-72
- Heitzman ER, Ziter FM Jr, Markarian B, McClennan BL, Sherry HT. Kerley’s interlobular septal lines: roentgen pathologic correlation. Am J Roentgenol Radium Ther Nucl Med. 1967 Jul;100(3):578-82.
- Koga T, Fujimoto K. Kerley’s A, B, and C lines. N Engl J Med 2009; 360:1539 [PDF]
- Sliker CW, Steenburg SD, Archer-Arroyo K. Emergency radiology eponyms: part 1-Pott’s puffy tumor to Kerley B lines. Emerg Radiol. 2013 Apr;20(2):103-11
eponymictionary
the names behind the name
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |