
![]()
LITFL Update 063
Sending you free open-access medical (FOAM) content from around the globe. We keep an eye on all the trends and best articles and share them with you so that you stay on top of your field.
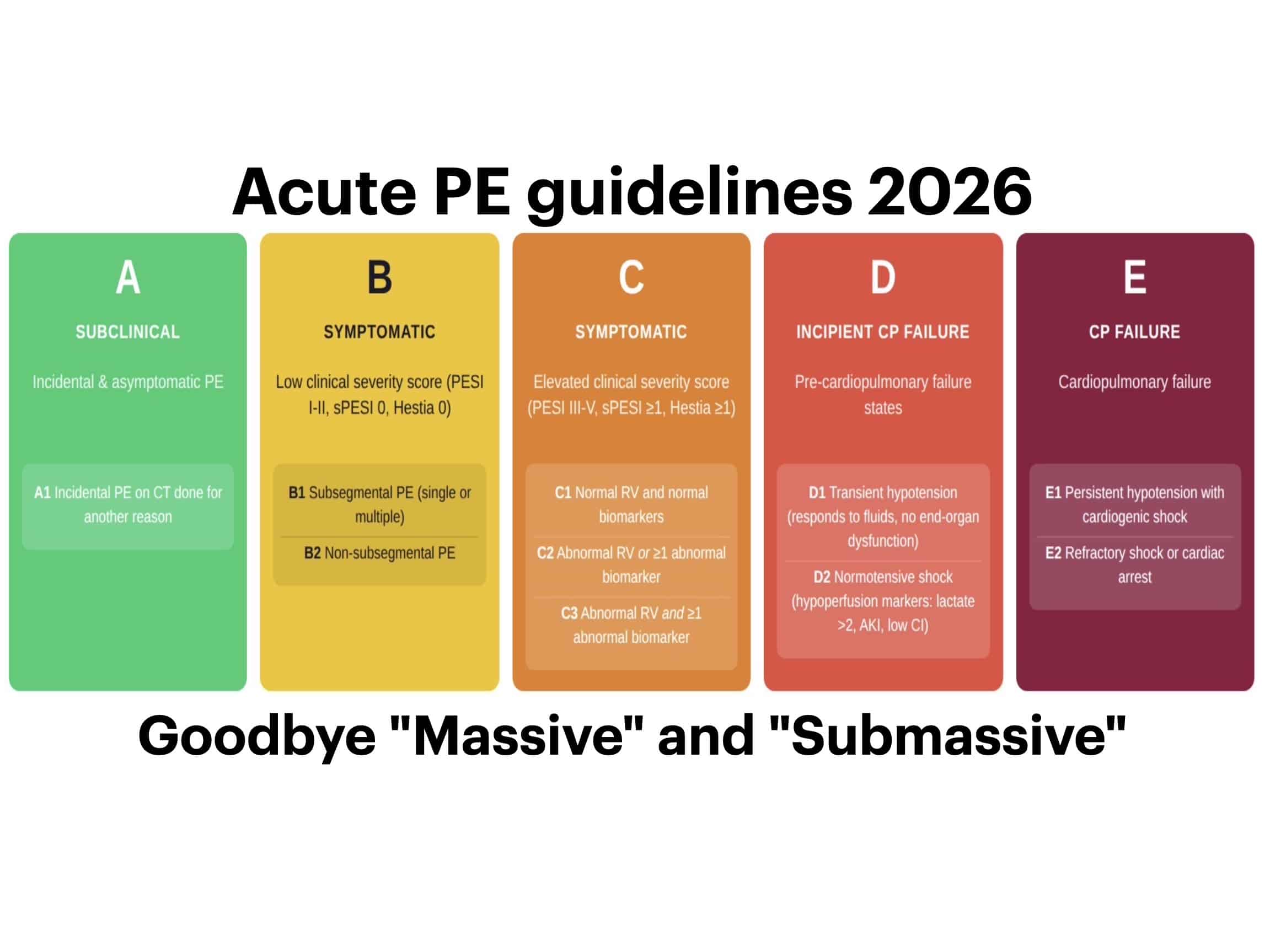
Goodbye “Massive” and “Submassive”: The 2026 Acute Pulmonary Embolism (PE) Guidelines have arrived, and drop a new A-to-E severity classification, promotes PERT teams to Class 1, and finally says it: DOACs over warfarin, LMWH over UFH. Here’s what you need to know.

MacGyver the Foley and control catastrophic bleeding: It’s 2 am when a 32-year-old male minding his own business in a kebab shop was stabbed in the left side of his neck. At the scene and en route to hospital, direct pressure was ineffective in controlling the profuse bleeding…
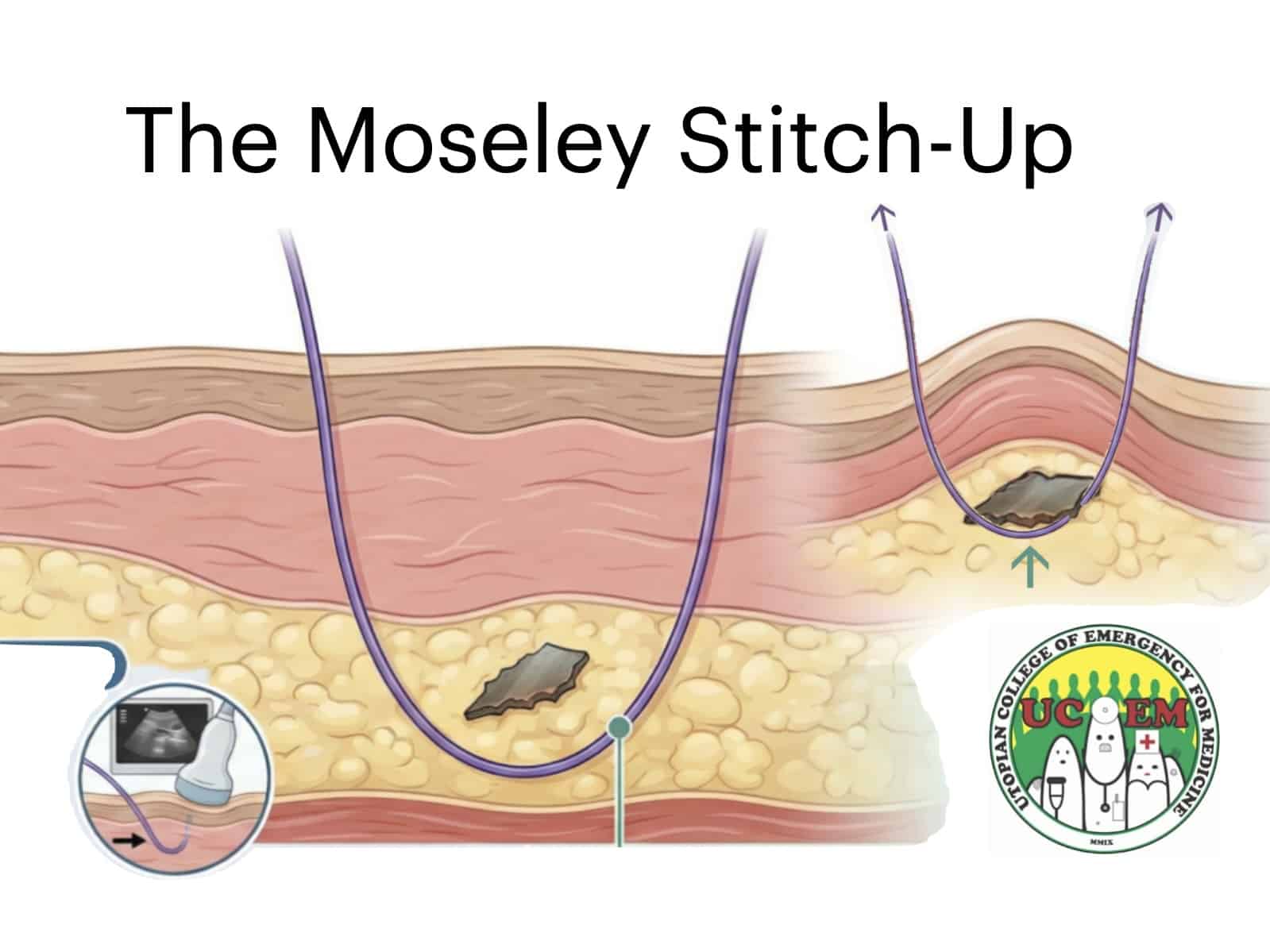
Eponymyth – The Moseley Stitch-Up™: Every clinician knows the profound frustration of the ultrasound-guided foreign body removal… the object darts around the subcutaneous tissues like a greased pig on ice. See the groundbreaking technique designed to end this game of subcutaneous Tom & Jerry.
Latest updates from the #FOAMed world
This podcast explores the critical care implications of meningitis through the lens of recent outbreaks, highlighting the need for early recognition and immediate antibiotics to improve outcomes. It emphasises transmission risks in social settings, the role of targeted vaccination (e.g. MenB), and the importance of public health messaging. Practical takeaways focus on maintaining high clinical suspicion, rapid escalation, and supporting patients, families, and communities during outbreaks.
Early trauma resuscitation has no single “correct” blood pressure target – it requires balancing bleeding control with brain and spinal cord perfusion. The blog reviews evolving evidence and guidelines, supporting permissive hypotension (~SBP 90 mmHg) in isolated haemorrhagic shock, while emphasising higher targets when neurological injury is present. It provides a pragmatic, bedside approach to navigating conflicting priorities in real-world polytrauma care.
This Emergency Medicine Cases update emphasises that cardiac arrest care still hinges on fundamentals – high-quality CPR, early defibrillation, and effective ventilation – but with a shift toward precision and performance. It highlights real-time CPR quality feedback, minimising pauses, smarter defibrillation strategies, and avoiding hyperventilation, while challenging rigid algorithms (like fixed 2-minute cycles) in favour of a more nuanced, patient- and physiology-driven resuscitation approach.
This blog highlights key caveats: only small volumes (2 units) were given, the study may be underpowered, and hospital care likely diluted any early differences. The takeaway – whole blood remains unproven, and outcomes may depend more on rapid haemorrhage control than the specific transfusion product.
LITFL Comms
Newsletter Updates
Emergency nurse with ultra-keen interest in the realms of toxicology, sepsis, eLearning and the management of critical care in the Emergency Department | LinkedIn |
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |
