
![]()
Lung ultrasound: Pleural effusion
The aims of ultrasound guided assessment of pleural effusion are:
- To determine and describe the size and site of the effusion.
- To mark the optimal site for drainage (and perform the procedure) if required.
- To characterize the effusion, noting echogenicity of the fluid, any loculations, solid masses and pleural disease.
- To observe and describe the underlying lung.
Understanding pleural effusion
The thoracic cage “unfolded”. The patient is sitting and there is a small pleural effusion on the left (right lung) and a large one on the right (left lung).
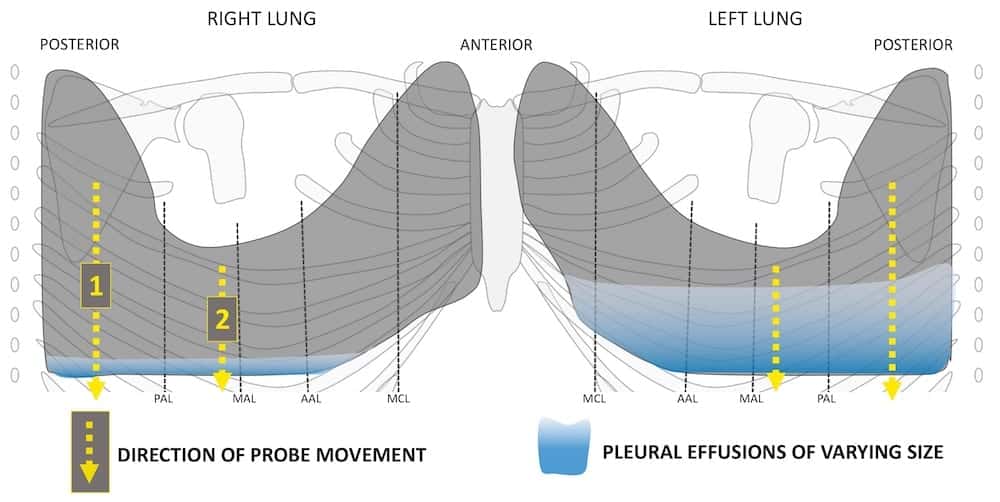
Pleural effusion collects at the most dependent position within each thoracic cavity.
- In the absence of an associated pneumothorax it forms a meniscus, tracking up the chest wall around the lung getting thinner and thinner until the two pleural surfaces meet.
- Pleural effusion is most easily examined if a patient can sit up. Then fluid collects at the lung bases and often below the lung lying on the diaphragm.
Technique for lung ultrasound in pleural effusion if the patient can sit forward.
The patient should be comfortable, ideally sitting on the edge of the bed with arms folded forwards and resting on a pillow on a stable surface just below shoulder height.
[1] Place the probe longitudinally on the posterior chest wall just medial to the blade of the scapula.
- Slowly slide the probe caudally watching the pleural line.
- Note the site of top of the effusion, the maximal depth, the depth to underlying lung, the diaphragm and its movement through the respiratory cycle, and the site of the costophrenic angle.
- To achieve a view that is not interrupted by rib shadows now repeat but rotate the probe’s upper end 45 degrees toward the spine and so the beam lies in an intercostal space. This will allow an uninterrupted view of the pleura, the effusion and underlying lung and will help with accurate characterisation
[2] Repeat the process laterally to determine the extent of the effusion and characterisitics of fluid, pleura and lung laterally.
Pleural effusion with the patient in different positions
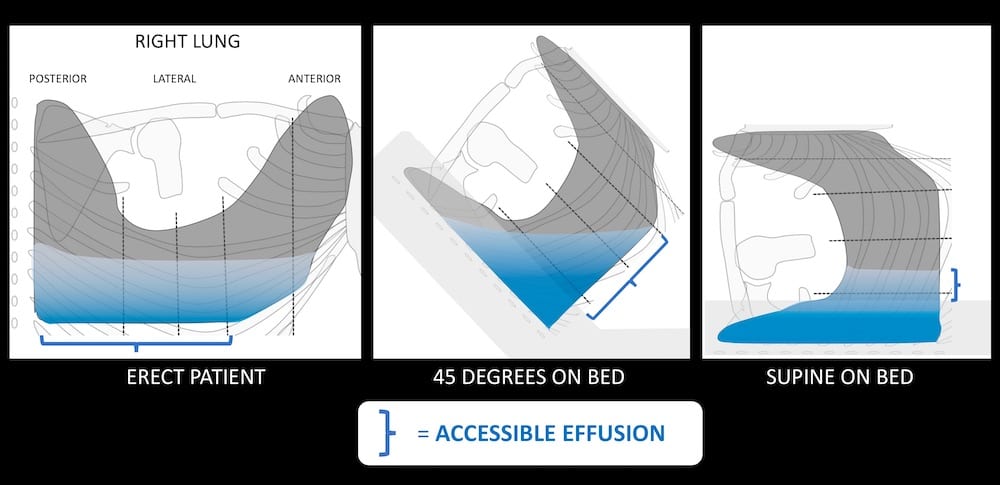
If the patient needs to rest back at 45 degrees fluid will collect in the dependent postero-inferior recess, and if they are lying flat it will collect posteriorly.
- In both these cases the approach will be lateral as the posterior chest is against the bed.
- The aims remain the same.
- Note the extent of the effusion, its maximal depth, the position of the diaphragm and its respiratory movement.
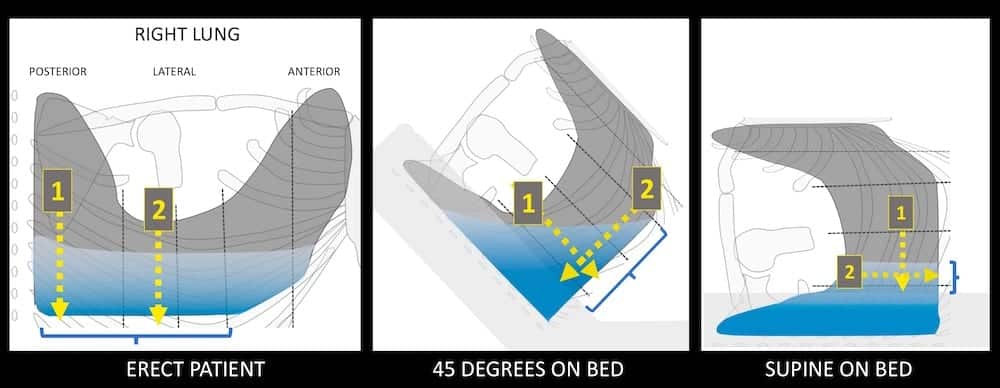
- Again I recommend placing the probe in the longitudinal axis relative to the thorax as I find this orientation best to determine the exact position of the diaphragm and to note its movement during repsiration.
- Next rotate the probe so it lies within an intercostal space to avoid rib shadows.
Potential Pitfalls
- Occasionally pleural masses are hypoechoic and masquerade as an effusion. Masses are usually rounded at the edges rather than tapering, they lack swirling internal fluid and collapsed waving underlying lung. They also often demonstrate internal vascularity on interrogation with colour Doppler.
- Subdiaphragmatic collections have been confused with pleural effusions.
Related Clinical Cases
- LITFL Ultrasound library
- LITFL Top 100 ultrasound cases
- LUNG ultrasound WORKED CASES
- LUNG ultrasound MODULES
ULTRASOUND LIBRARY
Modules

An Emergency physician based in Perth, Western Australia. Professionally my passion lies in integrating advanced diagnostic and procedural ultrasound into clinical assessment and management of the undifferentiated patient. Sharing hard fought knowledge with innovative educational techniques to ensure knowledge translation and dissemination is my goal. Family, wild coastlines, native forests, and tinkering in the shed fills the rest of my contented time. | SonoCPD | Ultrasound library | Top 100 | @thesonocave |
Thanks