
![]()
MacGyver the Foley
More Than Urine: Using a Foley Catheter to Control Catastrophic Bleeding
It’s 2 am, when a 32-year-old male was minding his own business in the kebab shop only to be stabbed to the left side of his neck. At the scene and en route to hospital direct pressure was ineffective in controlling the profuse bleeding.
On arrival to emergency, a right subclavian MAC line was inserted, 2g TXA administered, and massive transfusion protocol commenced.
Profuse bleeding continues from the wound and you suspect a carotid artery or internal jugular injury.
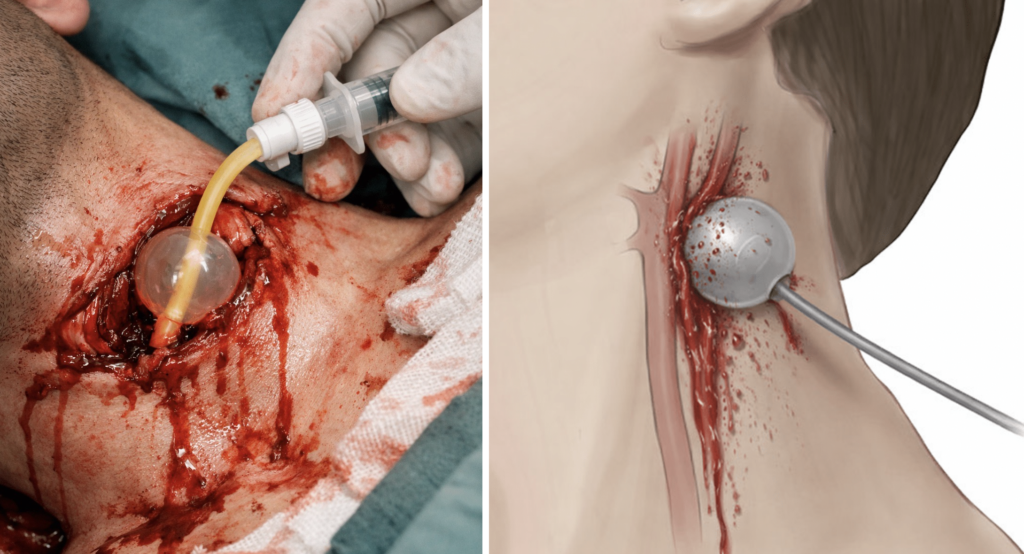
A 22Fr 3-way Foley catheter is inserted into the wound tract. The balloon is inflated with 40ml sterile water and gentle traction applied. The overlying wound is rapidly closed with 0 silk to maintain Foley placement.

Managing Non-Compressible Haemorrhage in ED
With haemorrhage controlled, the patient can be resuscitated, investigated with CT angiography and related studies as indicated, and then taken to definitive operative or endovascular management when major vascular injury is identified. Foley catheter balloon tamponade is a temporising manoeuvre that may also be definitive treatment in selected venous and minor arterial injuries.
Non-compressible haemorrhage remains a major cause of potentially preventable trauma death. Junctional injuries of the neck, axilla/subclavian region and groin are especially difficult because they are not readily controlled with direct pressure or standard limb tourniquets.
In this setting, Foley catheter balloon tamponade is one of several advanced bleeding control options that can provide early temporary haemorrhage control while definitive care is arranged.
Balloon catheter tamponade is not a first-line procedure. It is a simple, rapidly available bridge for selected penetrating junctional injuries when external compression is failing or anatomically limited.

The Principle: Balloon Tamponade
More than a century before contemporary Foley balloon tamponade in trauma, William E. Schroeder of Cook County Hospital described an inflatable rubber bag for penetrating liver haemorrhage. In 1906, Schroeder described controlling profuse haemorrhage from a gunshot wound of the liver by inserting and inflating a rubber bag within the wound tract.
An attempt was made to stop the profuse hemorrhage by gauze packing, which was unsuccessful, whereupon a small rubber bag was secured. The bag was inflated and the hemorrhage controlled.
Schroeder 1906
Modern trauma use follows the same basic principle: place the catheter into the wound tract without undue force, inflate the balloon until bleeding is controlled, clamp or knot the catheter to prevent back-bleeding, apply gentle traction, and secure the wound around the catheter to prevent expulsion.
Practical points
- Insert the catheter into the wound tract without creating a false passage.
- Inflate the balloon until resistance is felt and haemorrhage stops.
- Clamp or knot the catheter to prevent back-bleeding.
- Apply gentle traction.
- Secure the wound around the catheter with sutures or staples to prevent expulsion.
- If bleeding continues, consider a second catheter or immediate operative escalation.
- Once haemostasis is achieved, proceed to CTA and ancillary testing as indicated.
- Do not deflate the balloon on the ward; removal should occur in theatre with the team prepared to explore if rebleeding occurs.
Evidence Base
The available papers do not define a single optimal catheter type, balloon volume, or inflation fluid for every wound. Practically, the catheter should be chosen according to tract size and anatomy, with enough balloon volume to achieve tamponade without forcing the tract.
Scriba et al. from Groote Schuur Hospital analysed 628 patients with penetrating neck injury. 95 required Foley catheter balloon tamponade. Haemorrhage control was achieved in 92 of 95 patients (96.8%), 81.1% of catheters were inserted before arrival at the tertiary centre, and most patients required only one catheter. Major arterial injury still required selective operative or endovascular management, but venous and minor arterial injuries were often managed successfully with the catheter strategy.
They also discuss a controlled delayed-removal strategy. In patients without major arterial injury, catheter removal was generally attempted at 48–72 hours in the operating room. Rebleeding occurred in only 2 of 72 delayed removals, which is far lower than earlier series in which removal was attempted earlier.

Indications
Consider Foley catheter balloon tamponade when:
- There is penetrating neck haemorrhage not controlled with direct pressure.
- There is penetrating axillary/subclavian or groin haemorrhage in a junctional wound.
- The wound tract is deep or anatomically difficult to compress externally.
- Temporary haemorrhage control is needed while CTA, theatre, vascular surgery or endovascular management is organised.
- The aim is rapid bridging control in the ED and other settings where immediate definitive haemorrhage control is not yet available.
For the neck specifically, the best-supported pathway is haemorrhage control first, followed by selective imaging and further management rather than mandatory immediate neck exploration in every case.
Contraindications / Cautions
- Uncertain trajectory where blind advancement may create a false tract or worsen injury.
- Massive tissue destruction or a large open cavity where balloon tamponade is unlikely to be effective.
- Failure to control bleeding after placement.
- Lack of timely access to definitive operative or endovascular management.
- Any suspected associated aerodigestive injury or major arterial injury requiring urgent investigation after initial haemorrhage control.
Conclusion
Foley catheter balloon tamponade is a pragmatic temporising technique for selected penetrating junctional haemorrhage. The best clinical data in penetrating neck trauma suggest high initial haemorrhage-control rates and support delayed catheter removal in the operating room after imaging and planned reassessment.
That said, the evidence base remains largely observational. It is better described as a simple, accessible bridge within a broader haemorrhage-control strategy than as a definitive stand-alone solution for all cases.
References
- Schroeder WE. The progress of liver hemostasis—reports of cases (resection, sutures, etc). Surgery, Gynecology & Obstetrics 1906; 2(1): 52–61
- Feliciano DV. Balloons are not just for children. Trauma Surg Acute Care Open. 2021 Aug 4;6(1):e000808.
- Scriba M, McPherson D, Edu S, Nicol A, Navsaria P. An Update on Foley Catheter Balloon Tamponade for Penetrating Neck Injuries. World J Surg. 2020 Aug;44(8):2647-2655
- Vrancken SM, de Vroome M, van Vledder MG, Halm JA, Van Lieshout EMM, Borger van der Burg BLS, Hoencamp R, Verhofstad MHJ, van Waes OJF. Non-compressible truncal and junctional hemorrhage: A retrospective analysis quantifying potential indications for advanced bleeding control in Dutch trauma centers. Injury. 2024 Jan;55(1):111183.
Emergency Procedures
Emergency nurse with ultra-keen interest in the realms of toxicology, sepsis, eLearning and the management of critical care in the Emergency Department | LinkedIn |