
![]()
Mahogany Myoglobinuria
aka Unusual Urine 004
A 72 year old female is admitted following an emergency abdominal aortic aneurysm repair. The day after her surgery, the following biochemistry results are obtained:
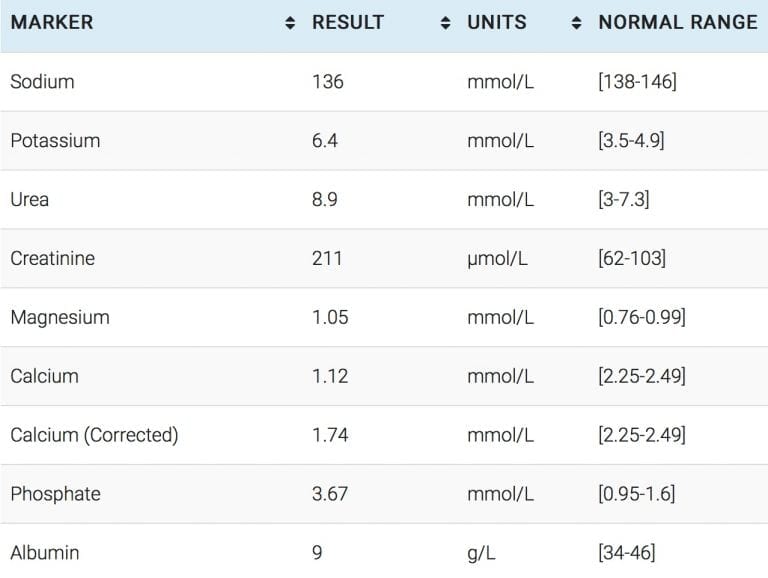
Describe the biochemical findings
Unusual Answer
Beyond the obvious (i.e. every value that fall outside of the reference range)…
The urea to creatinine ratio is low.
The expected creatinine based on the urea of 8.9 is approximately 89 – whereas, the actual creatinine is 211.
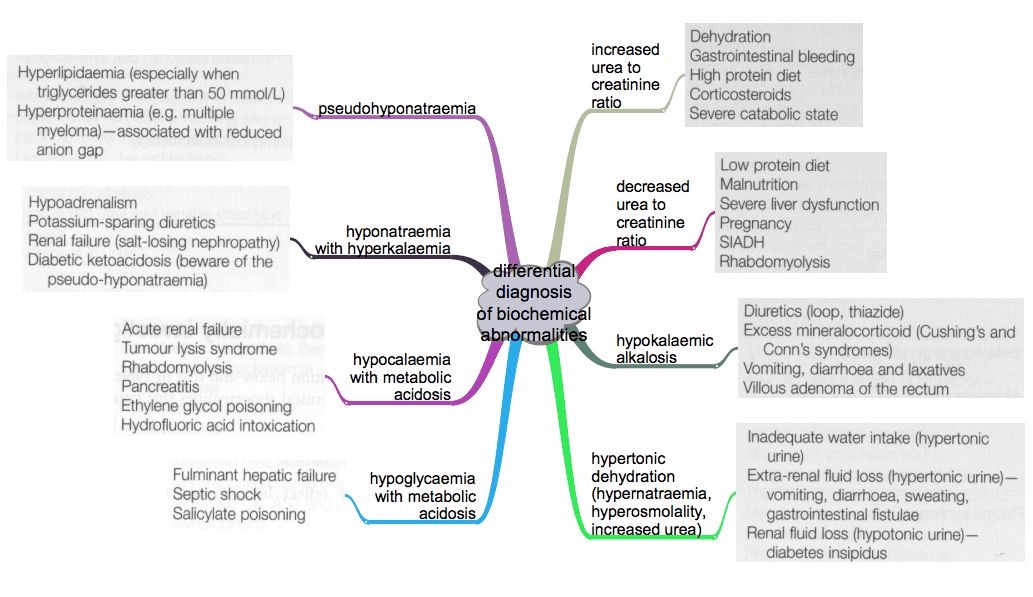
What are the causes of a reduced urea to creatinine ratio?
Unusual Answer
The causes of reduced urea to creatinine ratio include:
{kind=link}
- Low protein diet
- Malnutrition
- SIADH
- Pregnancy
- Severe Liver Dysfunction
- Rhabdomyolysis
The urine looks like this…

What is the likely diagnosis in this case?
Unusual Answer
Rhabdomyolysis
The diagnosis is effectively confirmed by a urine dipstick and urine microscopy.
Myoglobinuria can be inferred if a urinary dipstick is positive for blood when there are no red cells in the urine sediment. This is because, the dipstick test is unable to distinguish between myoglobin and haemoglobin.
How is this condition managed?
Unusual Answer
The management of rhabdomyolysis was recently reviewed in a clinical vignette in the New England Journal of Medicine.The recommendations in this review were as follows:
- aggressively correct hypovolaemia (a common problem due to sequestration of fluid in muscle)
- target a urine output of 3ml/kg/hr
- monitor serum potassium closely and treat hyperkalaemia with standard measures
- alternate each litre of saline with 1L litre of D5W plus 100mmol of bicarbonate if the urine pH is less than 6.5 (they suggest abandoning urinary alkalinisation if the urine pH does not rise after 4-6 hours of treatment or if symptomatic hypocalaemia develops)
- consider treatment with mannitol in a dose of up to 200g per day with a total accumulated dose of no more than 800g. Mannitol has dual roles of flushing nephrotoxic agents through the renal tubules and reducing muscle compartment pressures. They suggest that mannitol diuresis be abandoned if diuresis of >20ml/hr is not achieved or if the osmolar gap rises above 55mOsm/kg.
- commence renal replacement if there is treatment-resistant hyperkalaemia, a rapidly rising potassium, volume overload or a metabolic acidosis with a pH <7.1.
It is important to emphasise that the quality of evidence to guide treatment is very poor. Urinary alkalinisation and mannitol have a firm pathophysiological basis but no trial has demonstrated any particular benefit from either of these therapies.
What are the other causes of urine that looks like this?
Unusual Answer
- Haemoglobinuria
- Porphyria
- Bile pigments
- Food and drugs (levodopa, metronidazole, nitrofurantoin, iron, chloroquine and methyldopa all cause brown urine)
References
- Bosch X, Poch E, Grau JM. Rhabdomyolysis and Acute Kidney Injury N Engl J Med 2009; 361:62-7
Unusual Urine
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |
