
![]()
Metabolic Mayhem a Headache
aka Metabolic Muddle 003
An 87 year old female presented with a subarachnoid haemorrhage. GCS 8/15. A nasogastric tube was unable to be placed due to patient agitation. As a consequence, the patient was fasted for five days due to concern about swallowing.
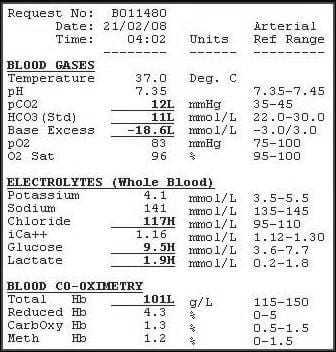
Arterial blood gas was subsequently obtained:
Questions
Q1. Describe the arterial blood gas
Answer and interpretation
- There is a metabolic acidosis with a high anion gap (HAGMA).
- The bicarbonate has decreased by more than the anion gap has increased which is due to a coexistent normal anion gap acidosis (NAGMA).
- There is a respiratory alkalosis. The pCO2 of 12mmHg is much lower than the respiratory compensation you would expect with this degree of metabolic acidosis (expected pCO2 = 1.5 * HCO3 +8 = 25 ).
The combination of these three abnormalities has led to relatively normal pH despite severe acid-base disturbance.
Q2. What are the causes of metabolic acidosis with raised anion gap and what is the likely cause here?
Answer and interpretation
There are two ways of remembering this.
The easy way is to remember ‘left total knee replacement’:
Lactate
Toxins
Ketones
Renal Failure
The more complicated way is CATMUDPILES:
Cyanide, Carbon monoxide
Alcoholic ketoacidosis
Toluene
Methanol, metformin
Uraemia
Diabetic Ketoacidosis
Phenformin, pyroglutamic acidosis, propylene glycol, paracetamol
Isoniazid, Iron
Lactic acidosis (many causes)
Ethanol, Ethylene glycol
Starvation, salicylates
The history suggests starvation ketoacidosis. There were ketones in the urine confirming this diagnosis.
Q3. What are the causes of normal anion gap acidosis and what is the likely cause here?
Answer and interpretation
The easy way to remember is OGRe:
Others (eg chloride)
GI loss of bicarb
Renal loss of bicarb

The more difficult way is to remember is USED CARP (the A and the R can be reversed – this is optional):
Ureteroenterostomy
Small bowel fistula
Extra Chloride
Diarrhoea
Carbonic anhydase inhibitors
Addisons disease
Renal tubular acidosis
Pancreatic fistula
Neurosurgeons like to give everyone lots of normal saline. The chloride is high.
The likely diagnosis is hyperchloraemic metabolic acidosis secondary to normal saline.
CLINICAL CASES
Metabolic Muddle
Intensivist in Wellington, New Zealand. Started out in ED, but now feels physically ill whenever he steps foot on the front line. Clinical researcher, kite-surfer | @DogICUma |