
![]()
Peritoneal Fluid Analysis
Peritoneal fluid (ascitic fluid) analysis
The peritoneum is a tough semi-permeable membrane lining abdominal and visceral cavities. it encloses, supports and lubricates organs within the cavity. Paracentesis is effectively the analysis of ‘Ascites’ – the abnormal accumulation of fluid within the abdomen.
- The peritoneum is important in osmoregulation
- Passive diffusion of water and solute (up to a certain size)
- Maintains osmotic and chemical equilibrium with blood and lymph
- Ascites develops either from:
- Increased accumulation
- Increased capillary permeability
- Increased venous pressure
- Decreased protein (oncotic pressure)
- Decreased clearance
- Increased lymphatic obstruction
- Increased accumulation
Cause
- Transudate (<30g/L protein) (Systemic disease)
- Liver (Cirrhosis)
- Cardiac e.g. RHF, CCF, SBE right heart valve disease and constrictive Pericarditis
- Renal failure
- Hypoalbuminaemia (nephrosis)
- Exudate (>30g/L protein) (Local disease)
- Malignancy
- Venous obstruction e.g. Budd-Chiari, Schistosomiasis
- Pancreatitis
- Lymphatic obstruction
- Infection (especially TB)
Analysate interpretation
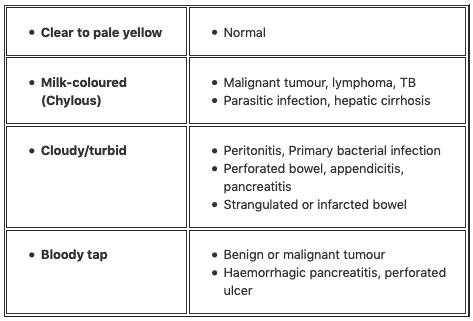
Gross appearance
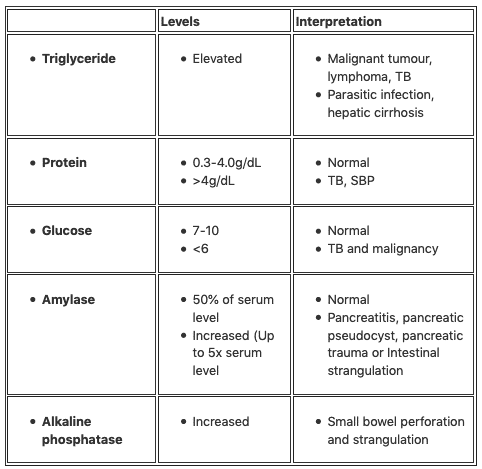
Paracentesis biochemistry
Exudate Serum:Ascites Ratios
- Evidence for these ascites:serum ratios is controversial
- Ascitic fluid protein/Serum Protein >0.5
- Ascitic Fluid LDH/Serum LDH >0.6
- Ascitic Fluid LDH >400
- Presence of any 2 of these three findings is usually associated with TB, Malignancy or Pancreatitis
- Absence of all three usually indicates hepatic cause
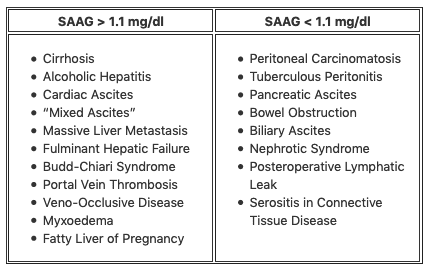
The Serum-Ascites Albumin Gradient (SAAG)
- The SAAG has become more favored in helping to characterize ascites fluid
- The concept surrounds oncotic-hydrostatic balance
- Simple calculation:
- Serum albumin – Ascites albumin= SAAG
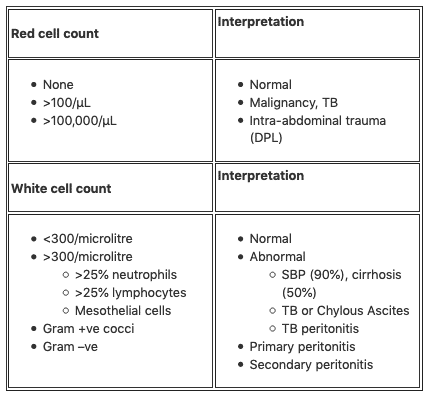
Microscopy and analysis
References and Links
- CCC – Ascitic fluid

Critical Care
Compendium
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |