
![]()
Sepsis Pathophysiology
OVERVIEW
Organisms
- Bacteria
-> Gram +ve’ cocci (staphylococci, streptococci)
-> Gram –ve bacilli (E.coli, Klebsiella, Pseudomonas aeruginosa) - Fungi (Candida)
- Viruses
- Parasites
Complex interaction between
- inciting microbe
- host immune response
- inflammatory pathway
- coagulation pathway
LPS = lipopolysaccharide
TRAF6 = TNF receptor-associated factor 6
NIK = nuclear factor-KB inducing kinase
NF-KB = nuclear factor-KB -> induction of immune response genes
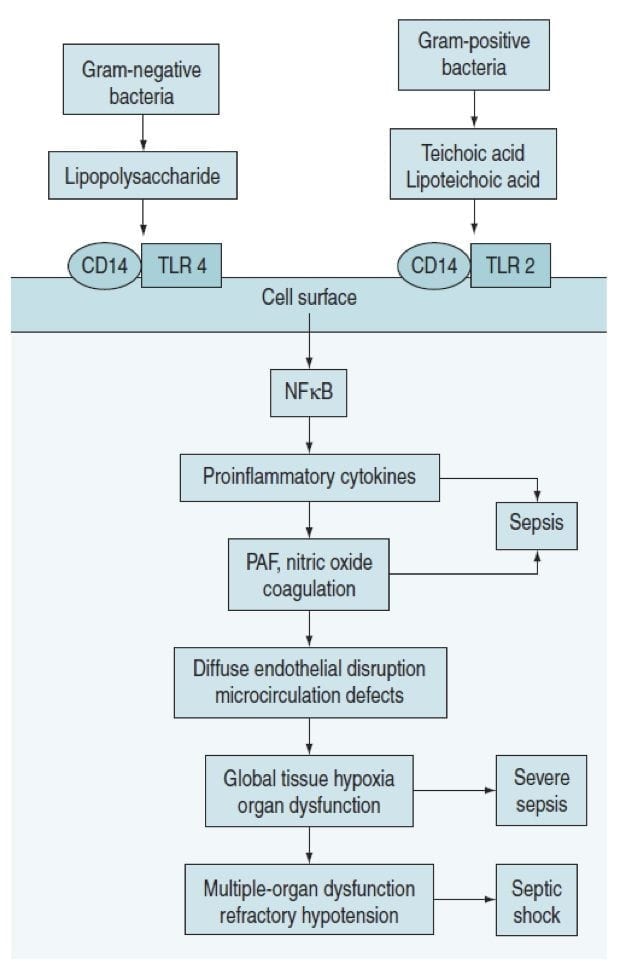
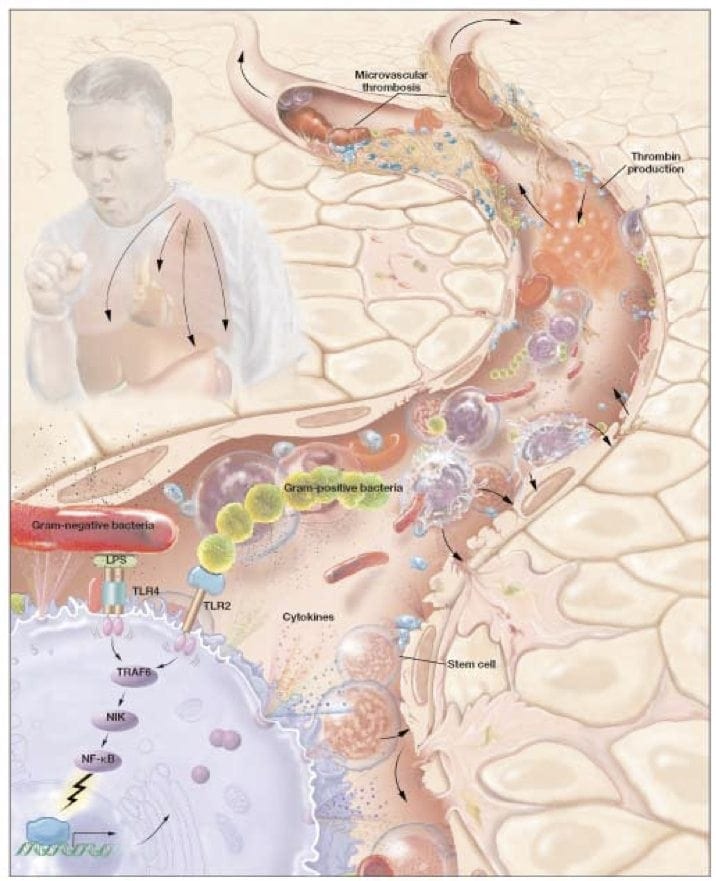
- pathogen binds to toll-like receptors (TLR’s) on surface of immune cells (monocytes)
- pro-inflammatory cytokines released
-> TNF-alpha, IL-1ß, IL-2, IL-6
-> increased NO synthase activity on endothelial cells - anti-inflammatory cytokines released
-> IL-4 and IL-10 - pro-coagulation cytokines
-> TF -> FVII release
-> endothelial injury and activation of coagulation cascade
- Inflammation –> neutrophil chemotaxis, increased capillary permeability, macrophage activation, lytic enzyme induction
- Coagulation –> fibrin production
- Fibrinolytic pathway suppression –> decreased APC and tPa activity -> decreased plasmin production
= microvascular thrombosis -> ischaemia -> organ dysfunction -> death
Pro-inflammatory mediators and pathways
- Cytokines – TNF, IL-1, IL-6, IL-8, IFN-y
- Coagulation pathways
- Macrophages, monocytes, neutrophils
- Endothelial cells
- Platelets
- Oxygen free radicals
- Proteases
- NO
Anti-inflammatory mediators
- IL-4, IL 10, IL-11, IL-13
- Transforming growth factor Beta
- CSF
- Soluble TNF receptors
- IL-1 receptor antagonist
- Natural anticoagulants
O2 delivery in Sepsis
- DO2 increased in septic shock from increased Q
- VO2 increased c/o raised tissue metabolic activity -> mitochondrial dysfunction
Lactic acidosis in Sepsis
- impaired regional microvascular blood flow & autoregulation
- mitochondrial dysfunction with impaired pyruvate oxidation
- excess catecholamines may impair hepatic lactate extraction (by reducing regional hepatic blood flow)
- lactate clearance is decreased because pyruvate dehydrogenase activity is reduced in both skeletal muscle and liver.
NB:
- tissue hypoxia may not be a major mechanism & NMR spectroscopy suggests that hyperlactaemia may occur without tissue hypoxia
- net lactate production from the hepatosplanchnic bed is uncommon in sepsis
References and Links
LITFL
- CCC — Sepsis definitions
Journal articles
- Andrades MÉ, Morina A, Spasić S, Spasojević I. Bench-to-bedside review: sepsis – from the redox point of view. Critical care. 15(5):230. 2011. [pubmed] [free full text]
- Angus DC, van der Poll T. Severe sepsis and septic shock. The New England journal of medicine. 369(9):840-51. 2013. [pubmed]
- Annane D, Bellissant E, Cavaillon JM. Septic shock. Lancet (London, England). 365(9453):63-78. 2005. [pubmed]
- Bosmann M, Ward PA. The inflammatory response in sepsis. Trends in immunology. 34(3):129-36. 2013. [pubmed] [free full text]
- Chertoff J, Chisum M, Garcia B, Lascano J. Lactate kinetics in sepsis and septic shock: a review of the literature and rationale for further research. Journal of intensive care. 3:39. 2015. [pubmed] [free full text]
- Landry DW, Oliver JA. The pathogenesis of vasodilatory shock. N Engl J Med. 2001 Aug 23;345(8):588-95. Review. PubMed PMID: 11529214.
- Rittirsch D, Flierl MA, Ward PA. Harmful molecular mechanisms in sepsis. Nat Rev Immunol. 2008 Oct;8(10):776-87. doi: 10.1038/nri2402. Review. PubMed PMID: 18802444; PubMed Central PMCID: PMC2786961.
FOAM and web resources
- EMCrit — Podcast 111 – Fluids in Sepsis, A New Paradigm by Paul Marik (2013)

Critical Care
Compendium
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |